Practice Essentials
The terms fibroxanthoma, nonossifying fibroma (NOF), fibrous cortical defect (FCD), and benign fibrous histiocytoma have all been used interchangeably in the radiology literature (see the images below). NOF and FCD, however, are considered to be 2 distinct lesions with respect to size and natural history. [1, 2, 3, 4, 5, 6] Fibroxanthoma is the preferred term for the NOF lesion because it more accurately reflects the underlying pathologic findings. In the literature, FCD has a longer list of pseudonyms, including metaphyseal fibrous defect, metaphyseal supracondylar cortical defect, and developmental defect. [1, 7, 8, 9, 10]
 Anteroposterior radiograph of the distal femur shows a solitary corticate lucent lesion within the posteromedial distal femoral cortex; this finding is consistent with a fibrous cortical defect.
Anteroposterior radiograph of the distal femur shows a solitary corticate lucent lesion within the posteromedial distal femoral cortex; this finding is consistent with a fibrous cortical defect.
 Coronal proton density–weighted MRI of the distal femur shows a fibrous cortical defect with a low signal intensity peripheral rim and its intracortical nature and subtle, central, intermediate signal intensity.
Coronal proton density–weighted MRI of the distal femur shows a fibrous cortical defect with a low signal intensity peripheral rim and its intracortical nature and subtle, central, intermediate signal intensity.
 Anteroposterior radiograph of the distal tibia shows a lobulated well-circumscribed nonossifying fibroma that is eccentrically located within the distal tibia metadiaphysis. Peripheral sclerotic border with a central lucency is typical of this lesion.
Anteroposterior radiograph of the distal tibia shows a lobulated well-circumscribed nonossifying fibroma that is eccentrically located within the distal tibia metadiaphysis. Peripheral sclerotic border with a central lucency is typical of this lesion.
FCDs have been mislabeled or described as cortical avulsive irregularities, subperiosteal or periosteal desmoid, a variant of periostitis ossificans, and cortical desmoid. The cortical desmoid—or cortical avulsive injury, as it is currently known—is believed to be separate from the cortical defect, and it has been related to repetitive stress at the attachment of the extensor tendon fibers along the linea aspera of the distal femur. [11]
Fibroxanthoma and FCDs are nonaggressive fibrous lesions of bone that are distinguished from one another historically by their size and natural history. Both are considered to be developmental defects and to be nonaggressive. They were first described by Lichtenstein and Jaffe in 1942, [12] and they typically occurred within the metaphysis of growing long tubular bones in children, most commonly about the knee. Controversy continues regarding the correct terminology and etiology of these lesions.
The distinction between FCD and fibroxanthoma is based on size and natural history. FCDs are asymptomatic, small (< 3 cm), eccentrically located, metaphyseal cortical defects; most of these spontaneously disappear. However, some evolve and enlarge into fibroxanthomas. Conversely, fibroxanthomas (>3 cm) are larger, eccentric, intramedullary lesions that abut the cortex; they have a typical, superficial, scalloping pattern in the adjacent cortex.
While these lesions also can heal spontaneously (with reactive bone filling in the central lucent fibrous tissue component), they can also persist, with interval growth that continues into adulthood. Typically, fibroxanthomas are asymptomatic. However, the larger lesions may become symptomatic, with a risk of pathologic fracture. Steiner suggested that these 2 lesions are secondary to cellular proliferation due to aberrations in local development. [13]
Clinical presentation
Typically, fibrous cortical defects (FCDs) are asymptomatic and are detected only incidentally on radiographs obtained for reasons other than the evaluation of FCD. Fibroxanthomas also are characteristically asymptomatic; however, in larger lesions, mild pain may occur secondary to radiographically undetected microfractures that may eventually lead to painful and radiographically evident pathologic fractures. [14] Although they are most commonly solitary lesions, multiple lesions have been described. Rare reports of multiple fibroxanthomas in patients with neurofibromatosis (5%) exist in the literature.
The presence of extraskeletal congenital anomalies (eg, café-au-lait spots, intellectual disability, hypogonadism or cryptorchidism, ocular abnormality, cardiovascular malformations) in association with multiple nonossifying fibroxanthomas constitute the clinical and radiologic spectrum known as Jaffe-Campanacci syndrome, which was first reported in 1983. [15, 16] In one series, Moser et al also noted that the coexistent osteochondromas can be present. [7]
Imaging modalities
Plain radiographic findings are virtually diagnostic of both fibrous cortical defects and nonossifying fibromas; most of these lesions have a characteristic location and appearance. If a discrepancy in appearance or age or an atypical associated symptom is present, advanced imaging (usually computed tomography [CT] or magnetic resonance imaging [MRI]) can be performed. [17, 18, 19, 20]
Although the radiographic findings usually are pathognomonic, the differential diagnosis includes the following: chondromyxoid fibroma; fibrous dysplasia, particularly if lesions are multiple and polyostotic (in comparison, fibrous dysplasia has a more central and unilateral location and more of a ground-glass appearance); osteoid osteoma (typically has a central nidus); bone abscess; periosteal chondroma; avulsive cortical irregularity or periosteal desmoid (saucerlike radiolucent defect in the cortex with adjacent sclerosis and periostitis); and desmoplastic fibroma.
Clinical history can be helpful in differentiating nonossifying fibromas from lesions that require further imaging. These lesions usually present asymptomatically, while pain, swelling, and tenderness are the more common presentation of aneurysmal bone cyst and chondromyxoid fibroma. [21] Large lesions of more than 50% of the width of the bone have been rarely reported. These lesions may present with pain and pathologic fracture and can recur following surgical intervention. [22]
Reports of soft-tissue desmoid or desmoplastic fibromas of bone have been noted only when the fibrous tissue in these lesions is examined at biopsy. Although much less common, consider giant cell tumor and aneurysmal bone cysts in the differential diagnosis of a large lobulated fibroxanthoma at radiographic study. However, both of these lesions are clearly distinguished at CT or MRI. A herniation pit also has been described in the differential diagnosis of fibrous cortical defect (FCD).
The cortical avulsive injury that occurs in adolescents has been noted more frequently. It often was and still is confused with FCD. At histologic evaluation, cortical avulsive injury has a nonspecific fibrous appearance with intermixed spicules of bone and healthy osteoblasts. Later findings indicated that the histologic features of the cortical avulsive lesion (characteristically located at the insertion of the tendon at the posteromedial cortex of the distal femur) included those of healthy tendon and interspersed bone and cartilage; therefore, this lesion is separate from FCD and secondary to repetitive trauma rather than being a true developmental defect.
Radiography
The imaging features of fibroxanthomas are pathognomonic. Typically, a metadiaphyseal, eccentric, ovoid or round, intramedullary geographic radiolucency, with a sharply marginated sclerotic rim of reactive bone and a scalloped contour, is present. The medullary rim typically is thicker than the cortical rim. While they initially appear near the physeal plate, they eventually appear further down within the diaphysis, following a normal growth pattern. The epiphysis is never affected. Larger lesions can appear multiloculated, with dimensions as large as 4-7 cm, with erosion of the endosteal surface of the cortex. [8, 19, 20, 23]
(See the radiographic images below.)
Anteroposterior radiograph of the distal femur shows a solitary corticate lucent lesion within the posteromedial distal femoral cortex; this finding is consistent with a fibrous cortical defect.
 Oblique (45°) radiograph of the distal femur best depicts the fibrous cortical defect. No soft-tissue mass or periosteal reaction is present.
Oblique (45°) radiograph of the distal femur best depicts the fibrous cortical defect. No soft-tissue mass or periosteal reaction is present.
 Anteroposterior image of the distal femur in an 8-year-old boy. Pain in the distal femur led to imaging. Cortical irregularity is present at the distal medial femoral metaphyseal cortex, which suggests cortical avulsive injury rather than fibrous cortical defect.
Anteroposterior image of the distal femur in an 8-year-old boy. Pain in the distal femur led to imaging. Cortical irregularity is present at the distal medial femoral metaphyseal cortex, which suggests cortical avulsive injury rather than fibrous cortical defect.
 Anteroposterior radiograph of the distal tibia shows a solitary, small, well-defined lucent lesion in the lateral distal tibial metadiaphysis that abuts the cortex. This finding is consistent with a benign fibrous cortical defect or nonossifying fibroma. Note the lack of multiple lobulations in this early lesion.
Anteroposterior radiograph of the distal tibia shows a lobulated well-circumscribed nonossifying fibroma that is eccentrically located within the distal tibia metadiaphysis. Peripheral sclerotic border with a central lucency is typical of this lesion.
Anteroposterior radiograph of the distal tibia shows a solitary, small, well-defined lucent lesion in the lateral distal tibial metadiaphysis that abuts the cortex. This finding is consistent with a benign fibrous cortical defect or nonossifying fibroma. Note the lack of multiple lobulations in this early lesion.
Anteroposterior radiograph of the distal tibia shows a lobulated well-circumscribed nonossifying fibroma that is eccentrically located within the distal tibia metadiaphysis. Peripheral sclerotic border with a central lucency is typical of this lesion.
 Anteroposterior radiograph of the distal tibia and fibula shows an expansile corticate lytic nonossifying fibroma within the distal fibular metaphysis with prominent expansion in the small tubular bones. A second nonossifying fibroma within the distal lateral tibial metaphysis in this patient with multiple nonossifying fibromas is noted. No clinical symptoms were present in this patient, and Jaffe-Campanacci syndrome could not be confirmed.
Anteroposterior radiograph of the distal tibia and fibula shows an expansile corticate lytic nonossifying fibroma within the distal fibular metaphysis with prominent expansion in the small tubular bones. A second nonossifying fibroma within the distal lateral tibial metaphysis in this patient with multiple nonossifying fibromas is noted. No clinical symptoms were present in this patient, and Jaffe-Campanacci syndrome could not be confirmed.
Since fibroxanthomas are thought to evolve from the fibrous cortical defect (FCD), the typical FCD appears similar but smaller, with the following defining features:
-
They usually are round or oval geographic radiolucencies that measure 1-3 cm.
-
They are located within the posteromedial aspect of the distal femoral cortex along the medial supracondylar ridge just proximal to the adductor tubercle.
-
A sharply marginated rim of reactive bone is identified where the lesion impinges on the medullary cavity.
-
No associated soft-tissue mass is present.
-
FCDs are best visualized in the anteroposterior (AP) oblique projection of the femur, with the limb in 20-40º external rotation.
While they typically are eccentric lesions within tubular bones, fibular lesions are an exception in that the entire diameter of the bone can be involved; this makes diagnosis slightly more difficult. Usually, fibroxanthomas are slow-growing lesions. Variations in size and density are secondary to interval growth and the natural resolution of the lesions; these processes include reactive bone formation, which can fill in and replace the central lucent defect over time.
This increase in sclerosis can be confusing to the observer and often is mistaken for fibrous dysplasia when it is present in the midst of the progressive changes. Initially, some of the lesions may be confused with neoplasms if one is not aware of the typical location and spectrum of their appearances over time. Knowledge of these characteristics is particularly important if periosteal reaction is present, since periosteal reaction occurs only with a pathologic fracture through the lesion.
These nonaggressive fibrous lesions have a characteristic location and appearance and are rarely confused with other lesions if the observer is aware of the spectrum of appearances over time. The degree of confidence is virtually certain in most cases; further imaging is required only if atypical symptoms or associated injuries are present.
Cortical avulsive injury to the distal posteromedial femur often has been confused with FCD. Usually, the former lesion has more cortical irregularity and is located at the direct insertion of the gastrocnemius muscle. They are more common in young athletes. These 2 may be part of a spectrum of the same type of lesion but, for now, are considered separately.
Computed Tomography
Advanced imaging usually is not required unless an atypical appearance or symptom is present. The characteristic lesion is eccentrically located, intramedullary, well marginated, and sclerotic, with a central lucency. Heterogeneous lucency and reactive sclerosis is identified at later stages in the case of the involuting fibroxanthoma. The central fibrous component has a nonspecific soft-tissue attenuation value; older lesions have a high attenuation value secondary to the reactive bone component.
CT images are useful because they can clearly depict the cross-sectional extent of bone involvement and the degree of cortical thinning, features that can help determine the risk of pathologic fracture.
The literature states that a tubular bone with a fibroxanthoma has a high risk for fracture if the lesion involves more than 50% of the width or if it extends more than 33 mm. If a fracture has occurred, a mild periosteal reaction may be present with subtle soft-tissue swelling; otherwise, no soft-tissue component is seen with fibroxanthomas, and the margins are very well demarcated.
Both lesions are fairly characteristic, and advanced imaging rarely is performed. The degree of confidence is 99%. With fibrous cortical defects (FCDs), the subtle apparent thickening of the cortical margin is noted with only subtle central cortical lucency because these lesions are very small in early disease. CT may help elucidate the irregular avulsive injury that is often confused with this lesion. Early differentiation between stress injuries caused by the adductor magnus muscle and the medial head of the gastrocnemius muscle, as well as clarification of the characteristic cortical defect, is possible with CT. When radiographic findings are not diagnostic, CT findings may obviate biopsy.
False-positive findings may include very small cortical avulsive irregularities. A small cortical osteoid osteoma may be confused as an FCD if the imaging sections are too thin and the nidus is not elucidated. However, clinical pain occurs with osteoid osteomas, which should not be confused with FCDs.
Magnetic Resonance Imaging
Usually, both fibroxanthoma and fibrous cortical defects (FCDs) are noted incidentally on images obtained for reasons other than evaluation of these lesions. Kransdorf et al described their characteristic low signal intensity on both T1- and T2-weighted spin-echo MRIs. [18] This finding is similar to that of other nonossified lesions that they reviewed. Low signal intensity on T2-weighted images was thought to represent hemosiderin deposits or large amounts of collagen, which are consistent with the fibrous tissue content.
(See the MRIs below.)
Coronal proton density–weighted MRI of the distal femur shows a fibrous cortical defect with a low signal intensity peripheral rim and its intracortical nature and subtle, central, intermediate signal intensity.
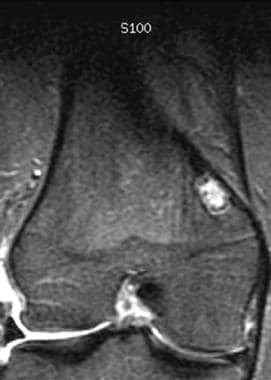 Coronal inversion-recovery MRI of the distal femur shows a fibrous cortical defect with a low signal intensity border and a central area with heterogeneous high signal intensity. No edema or cortical irregularity is present.
Coronal inversion-recovery MRI of the distal femur shows a fibrous cortical defect with a low signal intensity border and a central area with heterogeneous high signal intensity. No edema or cortical irregularity is present.
Because MRI is not commonly used in the evaluation of these lesions, data are limited. The degree of confidence with MRI alone is approximately 95%.
A peripheral hypointense rim represents the marginal sclerosis depicted on radiographs and the peripheral reactive sclerosis present at histologic evaluation. Bright areas can appear with sufficient cellularity. In a study by Jee et al, internal septa were noted in 95% of cases; these were correlated with subtle trabeculae depicted on the radiographs. [17]
Usually, MRI is not indicated in FCDs. However, study findings have shown that this intracortical lesion typically has low signal intensity on T1-weighted images and has increasing signal intensity on proton density– and T2-weighted images, which are consistent with their heterogeneous fibrous histologic characteristics. A rim of lower signal intensity represents the sclerotic border that abuts the medullary and cortical borders.
Other fibrous lesions can have the same signal intensity changes as those of fibroxanthoma and FCDs. However, the location and lack of pain should be helpful.
Nuclear Imaging
Minimal-to-mild accumulation of bone-seeking pharmaceutical agents (eg, technetium-99m [99mTc]) occurs and is indicative of a benign process. The intensity of the uptake is much less than that of active bone lesions.
In a child or adolescent, a typical eccentric region of agent uptake located a short distance from the physis of a tubular bone is diagnostic for fibroxanthoma in the appropriate setting. Fibrous cortical defects (FCDs) do not have uptake on bone scintigrams obtained with 99mTc. In children, this finding can be masked by the proximity of the lesion to the distal femoral epiphyseal plate, which itself has marked tracer uptake. [11, 24, 25, 2]
Cortical avulsive irregularities have increased tracer uptake in a location similar to that expected for an FCD. However, the former lesion has obvious uptake, unlike the usual pattern of no uptake in FCDs. Early osteosarcoma, particularly in the periosteal variant, can have 99mTc uptake within the distal posterior femur. Radiographic correlation helps in distinguishing between the aggressive lesion and benign FCD.
There are also FDG-PET/CT studies for fibrous cortical defects that have been published. [26, 6, 27]
-
Anteroposterior radiograph of the distal femur shows a solitary corticate lucent lesion within the posteromedial distal femoral cortex; this finding is consistent with a fibrous cortical defect.
-
Oblique (45°) radiograph of the distal femur best depicts the fibrous cortical defect. No soft-tissue mass or periosteal reaction is present.
-
Anteroposterior image of the distal femur in an 8-year-old boy. Pain in the distal femur led to imaging. Cortical irregularity is present at the distal medial femoral metaphyseal cortex, which suggests cortical avulsive injury rather than fibrous cortical defect.
-
Coronal proton density–weighted MRI of the distal femur shows a fibrous cortical defect with a low signal intensity peripheral rim and its intracortical nature and subtle, central, intermediate signal intensity.
-
Coronal inversion-recovery MRI of the distal femur shows a fibrous cortical defect with a low signal intensity border and a central area with heterogeneous high signal intensity. No edema or cortical irregularity is present.
-
Anteroposterior radiograph of the distal tibia shows a solitary, small, well-defined lucent lesion in the lateral distal tibial metadiaphysis that abuts the cortex. This finding is consistent with a benign fibrous cortical defect or nonossifying fibroma. Note the lack of multiple lobulations in this early lesion.
-
Anteroposterior radiograph of the distal tibia shows a lobulated well-circumscribed nonossifying fibroma that is eccentrically located within the distal tibia metadiaphysis. Peripheral sclerotic border with a central lucency is typical of this lesion.
-
Anteroposterior radiograph of the distal tibia and fibula shows an expansile corticate lytic nonossifying fibroma within the distal fibular metaphysis with prominent expansion in the small tubular bones. A second nonossifying fibroma within the distal lateral tibial metaphysis in this patient with multiple nonossifying fibromas is noted. No clinical symptoms were present in this patient, and Jaffe-Campanacci syndrome could not be confirmed.
-
Anteroposterior radiograph of the distal tibia and fibula demonstrates increased sclerosis and thickening of the peripheral rim of both lesions and increased heterogeneous central opacity; this finding is consistent with the natural growth pattern of these fibrous lesions.



