Background
Alkaptonuria, also called black urine disease, alcaptonuria, and black bone disease, is one of 4 disorders originally defined as an inborn error of metabolism by Archibald Garrod in his Croonian Lectures of 1902. [1] The hallmark of the disease is passage of urine that becomes black when left standing. Garrod identified a familial pattern of inheritance and concluded that an inherited biochemical abnormality must result in the passage of an abnormal intermediate in the urine. That Garrod conceived of an intermediate is remarkable given that virtually nothing was known of serial biochemical reactions in the metabolic disposal of nutrient substances at that time.
Pathophysiology
The defect lies in the catabolic pathway of tyrosine, which contains a parahydroxylated ring structure. In a poorly understood complex reaction, the enzyme phenylpyruvic acid oxidase is thought simultaneously to move the pyruvic acid side chain, to decarboxylate it, and to add an additional hydroxyl group to the ring. The product, homogentisic acid, is actually ortho-meta- dihydroxyphenylacetic acid. A deficiency of the hepatic enzyme homogentisate 1,2-dioxygenase (HGO) forces the accumulation of homogentisic acid, which is rapidly cleared in the kidney and excreted. [2, 3]
Upon contact with air, homogentisic acid is oxidized to form a pigmentlike polymeric material responsible for the black color of standing urine. Although homogentisic acid blood levels are kept very low through rapid kidney clearance, over time homogentisic acid is deposited in cartilage throughout the body and is converted to the pigmentlike polymer through an enzyme-mediated reaction that occurs chiefly in collagenous tissues [4] . As the polymer accumulates within cartilage, a process that takes many years, the normally transparent tissues become slate blue, an effect ordinarily not seen until adulthood.
The earliest sign of the disorder is the tendency for diapers to stain black. Throughout childhood and most of early adulthood, an asymptomatic, slowly progressive deposition of pigmentlike polymer material into collagenous tissues occurs.
In the fourth decade of life, external signs of pigment deposition, called ochronosis, begin to appear. See the image below.
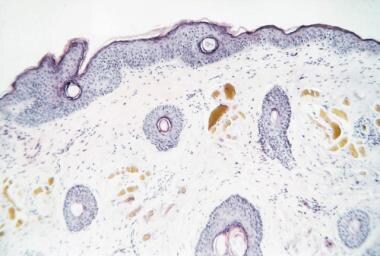 Upon microscopic examination, amber-colored, oval-shaped structures are detected in the mid-to-upper dermal tissues (hematoxylin and eosin, original magnification X40).
Upon microscopic examination, amber-colored, oval-shaped structures are detected in the mid-to-upper dermal tissues (hematoxylin and eosin, original magnification X40).
The slate blue, gray, or black discoloration of sclerae and ear cartilage is indicative of widespread staining of the body tissues, particularly cartilage. The hips, knees, and intervertebral joints are affected most commonly and show clinical symptoms resembling rheumatoid arthritis. Because of calcifications that occur in these sites, however, the radiologic picture is more consistent with osteoarthritis. Recently, ocular pigment deposition has been recognized, with adverse implications for vision. [5]
Despite many speculations that this polymer deposition is associated with cardiac pathology, no reports of mortality directly related to the homozygous state for alkaptonuria exist. Reports exist of calcification and stenosis of the aortic annulus leading to coronary artery disease, and the risk of myocardial infarction is higher than normal in older patients with ochronosis. [6]
Molecular analysis of the HGO gene shows a wide spectrum of mutation. Although no correlation has so far been made between the molecular nature of the HGO mutation and its clinical phenotype, the wide variability of mutational phenomena could certainly help explain the clinical variability in this disease. Approximately 130 separate mutations have thus far been reported.
Epidemiology
Frequency
United States
As Garrod suggested, alkaptonuria is an autosomal recessive genetic trait, although an autosomal dominant transmission pattern in 3 generations in a nonconsanguineous family has been reported. [7] The true frequency of alkaptonuria cannot be given with certainty for numerous reasons. These include the fact that newborn screening for alkaptonuria is much less widely practiced than that for phenylketonuria. Guidelines for phenylketonuria screening have been well established. [8]
Also, some carriers express 50% or more of normal enzyme activity and do not manifest abnormal findings even with tyrosine loading. To further complicate this picture, reports in the literature indicate wide variability in incidence, particularly where gene pools are highly restricted. In certain areas, an incidence rate as high as 1 in every 25,000 live births has been reported; worldwide it is certainly far lower.
Mortality/Morbidity
Life expectancy is normal; however, associated morbidity can be significant. Early involvement of the intervertebral discs at the thoracic and lumbar levels is very common, occurring in approximately 50% of affected individuals. Typically, significant back pain begins from age 30 years. The large joints (knee, shoulder and hip) are very frequently involved; at least half of all patients undergo joint replacement by the middle of the sixth decade of life. Achilles tendon involvement is also common and may result in tearing. Involvement of the aortic leaflets, mitral valve leaflets, or both is common, and calcifications of the coronary arteries occurs in one half of all patients prior to age 60 years.
Sex
The distribution of this disease is equal in males and females because it is an autosomal recessive or autosomal dominant trait. Males tend to have an earlier onset of arthritic symptoms with a greater degree of severity than females, although the reason for this difference is unclear.
Age
Because alkaptonuria is a genetic disorder, the deficiency of the HGO enzyme is present from conception. Clinical symptoms, aside from dark-stained diapers, are generally present only after the third decade of life.
-
Upon microscopic examination, amber-colored, oval-shaped structures are detected in the mid-to-upper dermal tissues (hematoxylin and eosin, original magnification X40).






