Practice Essentials
External auditory canal (EAC) atresia (EACA) is a rare congenital disorder. Accurate counseling and referral for these children and their families demands an appreciation of the range of management options and indications for intervention. This article reviews the history, etiology, and epidemiology of EACA, as well as the clinical care of children with this condition.
EACA was first described in Western medicine by Paulus of Aegina in the seventh century CE. Paulus recommended simple incision for opening the atretic canal. Later, physicians used a hot iron probe to maintain canal patency after incising the atresia. The first operation to correct an atresia of the EAC was performed in 1882 by Kiesselbach. Unfortunately, the operation left the child with a facial-nerve paralysis. In 1914, Page reported on a series of eight patients who underwent operation. Of these eight patients, five had a subjective improvement in their hearing after surgery.
In the early 20th century, techniques for correction of the atretic external canal involved opening the antrum and aditus of the ear and lining the cavities with a skin graft. In these surgeries, the atretic bony plate was untouched, and the resulting hearing improvement was poor. In the late 20th century and early 21st century, improved radiologic and audiologic assessments coupled with improvements in surgical technology, such as the operating microscope and facial-nerve monitoring, have resulted in good surgical success rates for properly chosen patients with EACA.
The future of medical and surgical interventions for patients with EACA is exciting and includes such novel approaches as computer-aided surgery and critical reviews of past surgical results, with further attempts to increase success rates and minimize morbidity.
Pathophysiology
The EAC is composed of medial bony and lateral cartilaginous portions. The bony component changes from half of the length of the tubular EAC in children to two thirds of the length of the tubular EAC in adults.
The lateral soft-tissue portion of the EAC begins to form at 26-28 weeks' gestation, when the epithelial plug arising from the first branchial cleft begins to canalize. During month 6 of development, the medial bony portion is created out of the temporal bone's mesenchymal condensation. As canalization occurs, the mastoid separates from the mandible and grows posteriorly and inferiorly. The facial nerve travels along with the posteroinferior growth of the mastoid, taking its final course from the middle ear and mastoid and exiting the skull base inferior to the EAC.
Congential atresia of the EAC is caused by a failure of canalization of the epithelial plug portion of the first branchial cleft. Persistence of the tympanic ring results in a bony atresia plate at the level of the tympanic membrane. Ossicular malformations may be seen as they arise from the first branchial cartilage (ie, Meckel cartilage).
Failure of the EAC to canalize means that sound cannot reach the tympanic membrane; thus, a conductive hearing loss results (see the images below). Concomitant ossicular malformations may result in additional conductive hearing loss. In addition, 11-47% of patients also have a sensorineural hearing loss in the affected ear.
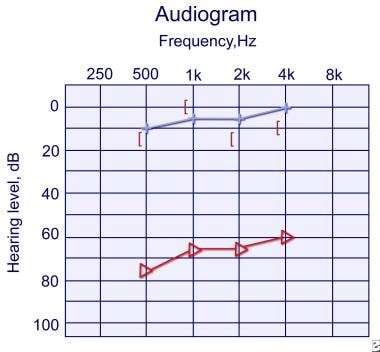 Audiogram of 5-year-old girl with right unilateral external auditory canal atresia (EACA) is shown. Audiogram demonstrates right conductive hearing loss, indicated by difference in hearing levels between red triangles and black brackets. Left ear hearing levels shown by the blue line are normal. This child demonstrated good function at home and in preschool and did not require intervention at this point.
Audiogram of 5-year-old girl with right unilateral external auditory canal atresia (EACA) is shown. Audiogram demonstrates right conductive hearing loss, indicated by difference in hearing levels between red triangles and black brackets. Left ear hearing levels shown by the blue line are normal. This child demonstrated good function at home and in preschool and did not require intervention at this point.
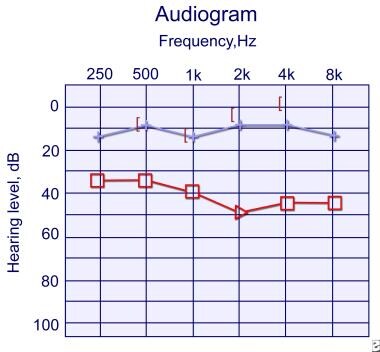 Audiogram 1 year later of same child as in preceding image. Functioning in kindergarten continues to be excellent, and patient has noticed hearing improvement at home. Physical examination shows pinpoint opening at external auditory canal (EAC) now, and this audiogram confirms improved hearing in right ear compared with prior audiogram (see image above). Her right conductive hearing loss is shown by distance between black brackets and red triangles.
Audiogram 1 year later of same child as in preceding image. Functioning in kindergarten continues to be excellent, and patient has noticed hearing improvement at home. Physical examination shows pinpoint opening at external auditory canal (EAC) now, and this audiogram confirms improved hearing in right ear compared with prior audiogram (see image above). Her right conductive hearing loss is shown by distance between black brackets and red triangles.
EACA may be seen with microtia (ie, maldevelopment of the external ear). The auricle develops from ectodermal condensations and mesodermal condensations (referred to as the hillocks of His) at 5 weeks' gestation.
Case reports have detailed duplication anomalies of the first branchial cleft occurring in conjunction with a congenital aural atresia. It is therefore important for the evaluating physician to keep in mind that EACA and duplication anomalies can be present in the same patient and that both may have to be simultaneously addressed (surgically).
Etiology
The precise etiology of the failure of EAC canalization is not known. Associations have been postulated between EACA and low birth weight, intrauterine trauma, toxins, or infection. Genetic defects are being identified for several craniofacial anomalies. Because of the importance of future genetic studies, serum must be obtained and banked for eventual genetic testing.
Epidemiology
United States and international statistics
According to Jahrsdoerfer, the incidence of ear malformations in New York City from 1952-1962 was 1 in 5800 births. [1] In one year of this study, the incidence of EACA was 1 in 8000 births.
EACA is rare in persons with a normal pinna. The incidence of EACA with concurrent microtia is 1 in 10,000-20,000 live births. Unilateral EACA is three to six times more likely to occur than bilateral EACA. The right ear is more often involved than the left ear. Family histories positive for EACA are noted in 14% of patients.
Age- and sex-related demographics
EACA occurs with a normal pinna or with an abnormal pinna (ie, concomitant microtia). When the atresia occurs in the setting of a normal pinna, the average age of diagnosis is 2.5 years. However, when EACA occurs with abnormal development of the pinna, the average age of diagnosis is 3.5 years.
EACA occurs more often in males than in females.
Prognosis
Hearing is measured in dB; a normal hearing level is considered to be between 0 and 15-20 dB for children. Higher measurements indicate sounds must be louder for a person to perceive them. A jet plane, for example, has a sound-pressure level (SPL) of approximately 110 dB. Children with ear infections usually have a 40-dB hearing level.
In a series of 16 patients published in 1988, Lambert obtained a speech-reception threshold (SRT) or hearing threshold of 30 dB or greater in 67% of the operated ears. [2] In De la Cruz's larger study of 302 ears, 73% of patients had a residual hearing deficit of 30 dB or less at 6-month follow-up. [3] Jahrsdoerfer reported that 73% of 90 patients who had scores higher than 6 according to his grading system (see Surgical Care) and underwent operation achieved an SRT less than or equal to 25 dB. [4]
The House Ear Institute published its results in 2004. [5] It compared modifications in its technique with its previous surgical technique. The new modifications included the use of the argon laser, thinner split-thickness skin grafts, Silastic sheets, and Merocel wicks in the EAC. With these modifications, hearing results were closure of the air-bone gap to 30 dB or less in 63% of patients, with a long-term postoperative air-bone gap of 30 dB or less in 50% of patients. Ossicular chain refixation occurred in only 4% of these patients.
According to Wetmore et al, Krowiak and Grundfast believe that the standard of care when surgically correcting an atretic EAC includes creation of a patent EAC, resolution to a hearing level of 25 dB or less, and closure of the air-bone gap. [6]
For unilateral conductive hearing loss due to unilateral EACA, Glasscock et al explain to patients that if surgery is successful, they should be able to listen to stereo music, tell the directionality of sound, and hear better in a noisy environment. [7] Patients are told not to expect improved hearing after surgery in a quiet place or in one-to-one conversation.
An excellent study that included a cost analysis of surgery versus hearing aids found that "even with significant investments in EAC reconstruction, most patients still required some form of amplification." [8, 9] Cost analysis suggests that osteointegrated bone-conduction devices may have an economic advantage over surgical intervention.
-
Photograph of right ear in patient with unilateral external auditory canal atresia is shown. Note relatively normal pinna and thumbprint concha.
-
Audiogram of 5-year-old girl with right unilateral external auditory canal atresia (EACA) is shown. Audiogram demonstrates right conductive hearing loss, indicated by difference in hearing levels between red triangles and black brackets. Left ear hearing levels shown by the blue line are normal. This child demonstrated good function at home and in preschool and did not require intervention at this point.
-
Audiogram 1 year later of same child as in preceding image. Functioning in kindergarten continues to be excellent, and patient has noticed hearing improvement at home. Physical examination shows pinpoint opening at external auditory canal (EAC) now, and this audiogram confirms improved hearing in right ear compared with prior audiogram (see image above). Her right conductive hearing loss is shown by distance between black brackets and red triangles.
-
CT scan in axial plane of right unilateral external auditory canal (EAC) atresia (EACA) is shown. Right EAC, to left of this photo, is not developed in comparison with normally developed left EAC. Image is slightly tilted in horizontal plane.
-
CT scan showing unilateral auditory canal atresia in coronal section of right ear. No ear canal is seen to left of this picture (patient's right).





