Practice Essentials
Traumatic penile injury can be due to multiple factors. Penile fracture, penile amputation, penetrating penile injuries, and penile soft tissue injuries are considered urologic emergencies and typically require surgical intervention.
The goals of treatment for penile trauma are universal: preservation of penile length and erectile function, and maintenance of the ability to void while standing.
Traumatic injury to the penis may concomitantly involve the urethra. [1, 2] Urethral injury and repair is beyond the scope of this article but details can be found in Urethral Trauma.
Penile fracture
Penile fracture is the traumatic rupture of the corpus cavernosum. Traumatic rupture of the penis is relatively uncommon and is considered a urologic emergency. [3]
Sudden blunt trauma or abrupt lateral bending of the penis in an erect state can break the markedly thinned and stiff tunica albuginea, resulting in a fractured penis. One or both corpora may be involved, and concomitant injury to the penile urethra may occur. Urethral trauma is more common when both corpora cavernosa are injured. [4]
Penile fracture can usually be diagnosed based solely on history and physical examination findings; however, in equivocal cases, diagnostic cavernosography, penile ultrasound by an experienced ultrasonographer, or MRI should be performed. Concomitant urethral injury must be considered; therefore, preoperative retrograde urethrographic studies should generally be performed. See the images below.


Penile amputation
Penile amputation involves the complete or partial severing of the penis. A complete transection comprises severing of both corpora cavernosa and the urethra. Amputation of the penis may be accidental but is often self-inflicted, especially during psychotic episodes in individuals who are mentally ill. See the image below.
Penetrating injury
Penetrating injury is the result of ballistic weapons, shrapnel, or stab injuries to the penis. Penetrating injuries are most commonly seen in wartime conflicts and are less common in civilian medicine. Penetrating injuries can involve one or both corpora, the urethra, or penile soft tissue alone. In the setting of ballistic weapon injuries, concomitant trauma to adjacent structures, such as the scrotum, testicles, and gastrointestinal organs, should be considered and ruled out. See the image below.

Penile soft tissue injury
Penile soft tissue injury can result through multiple mechanisms, including infection, burns, human or animal bites, and degloving injuries that involve machinery. The corpora, by definition, are not involved.
Background
History of the Procedure
Historically, conservative management was considered the treatment of choice for penile fractures. Conservative therapy consisted of cold compresses, pressure dressings, penile splinting, anti-inflammatory medications, fibrinolytics, and suprapubic urinary diversion with delayed repair of urethral injuries. This concept has fallen into disfavor because of the high complication rates (29-53%) of nonoperative therapy. Complications of conservative management included the following [5, 6] :
-
Missed urethral injury
-
Penile abscess
-
Nodule formation at the site of rupture
-
Permanent penile curvature
-
Painful erection
-
Painful coitus
-
Erectile dysfunction
-
Corporourethral fistula
-
Arteriovenous fistula
-
Fibrotic plaque formation
Relevant Anatomy
The penis is divided into 3 parts. The root lies under the pubic bone and provides stability when the penis is erect. The body comprises the major portion of the penis and is composed of 2 cavernosal bodies and a corpus spongiosum. The urethra traverses the corpus spongiosum to exit through the meatus. The 2 cavernosal bodies (ie, corpus cavernosa, erectile bodies) produce erections when filled with blood. The glans is the distal expansion of the corpus spongiosum. The loose skin of the prepuce normally covers the glans of an uncircumcised penis.
The penis is innervated by the left and right dorsal nerves, which are the main sensory nerve supply. These nerves are typically located at the 10- and 2-o'clock positions, but, in reality, their locations significantly vary. Care must be taken with surgical exploration of any penile injury to avoid iatrogenic injury to the dorsal nerves. The penis is also innervated by branches of the pudendal nerve.
The penis is a highly vascular organ and is supplied by the internal pudendal artery. The internal pudendal artery rises from the internal iliac artery (ie, hypogastric artery), which then branches into the deep artery of the penis, the bulbar artery, and the urethral artery. The deep artery of the penis becomes the cavernosal arteries, which supply the entire corpus cavernosum. The urethral artery supplies the glans penis and corpus spongiosum. The bulbar artery supplies the bulbar urethra and the bulbospongiosus muscle.
Pathophysiology
The penis is composed of 3 bodies of erectile tissue: the corpus cavernosum (left and right) and the corpus spongiosum. Both corpora cavernosa are contained by the tunica albuginea. All three corpora are surrounded individually by the Buck fascia.
All three corporal cylinders are capable of considerable enlargement with sanguineous engorgement during normal erection. The corpora cavernosa are composed of sinusoids that fill with arterial blood during erection.
The internal pudendal arteries provide the blood supply to the penis and the urethra. Each artery divides into the dorsal penile artery, the cavernosal artery, and the bulbourethral artery. The cavernosal artery supplies the corpus cavernosum.
Penile fracture
In the flaccid state, injury to the penis is rare because of the mobility and flexibility of the organ. During an erection, the arterial inflow to the penis causes the erectile bodies to enlarge longitudinally and transversely. This causes the flaccid penis to become fully erect and less mobile.
As the penis changes from a flaccid state to an erect state, the tunica albuginea thins from 2 mm to 0.25-0.5 mm, stiffens, and loses elasticity. The expansion and stiffness of the tunica albuginea impede venous return and are responsible for maintaining tumescence during male erection.
Sudden direct trauma to the penis or an abnormal bending of the erect penis can cause a 0.5-4 cm transverse tear of the tunica albuginea, with injury to the underlying corpus cavernosum. Oblique or irregular tears are less common, but have been reported. The trauma usually results in injury to one corpus cavernosa (usually at the ventrolateral location), but both can be involved. Urethral injurymay also occur.
Penetrating injury
The penis is somewhat resistant to penetrating injury owing to its location and relative mobility. The penis is shielded by the surrounding bony pelvis posteriorly and upper thighs laterally, which helps prevent injury.
Penile soft tissue injury
The penis is particularly susceptible to avulsion injuries. The overlying skin of the penis is loose and elastic, as it must be highly mobile to accommodate both the rigid and flaccid state of the penis. This loose base predisposes the skin to be ripped easily from the penis.
Etiology
Penile fracture
A meta-analysis on penile fractures showed that the most common causes are sexual intercourse (46%), forced flexion (taqaandan) (21%), masturbation (18%) and rolling over (8.2%). [7] The most common mechanism of injury is when the penis slips out of the vagina and strikes against the symphysis pubis or perineum. Penile fracture is more likely when the partner is on top but can occur in any coital position. [8]
Penile amputation
Penile amputation is frequently self-inflicted, as a result of mental illness. In the Western world, as many as 87% of penile amputations are due to mental illness. Most of these patients (51%) have acutely decompensated schizophrenia. The literature reports a high rate of associated gender identity in nonpsychotic occurrences; most of these amputations result from an attempt at gender conversion.
Cases of assault are also reported. A rash of these attacks occurred in Thailand during the 1970s, when a large number of enraged wives amputated the penises of their adulterous husbands.
Penetrating injury
Most penetrating penile injuries occur during wartime. As solid-organ abdominal injuries and subsequent death rates have been reduced with the use of body armor in modern warfare, the frequency of penetrating genital injuries has increased. This is because of two factors. The first is that body armor does not traditionally cover the genitals. The second is that genital injuries were likely underreported in previous wars because unprotected individuals tended to die of massive abdominal injuries. Extraction of injured soldiers from the combat theater and improvements in the treatment of trauma patients have also increased survival rates, leading to increased reporting of injuries to the penis.
Penile soft tissue injury
Avulsion injuries to the penis are typically due to entrapment of the penile skin within the clothing. The clothing is caught on moving machinery, such as motorcycles or farm implements, which rends the soft tissue from the stronger underlayer of the tunica albuginea.
Epidemiology
Penile fracture
The frequency of penile fracture is likely underreported in the published literature. Trauma during sexual relations is responsible for approximately one third of all cases; the female-dominant position is most commonly reported. The mechanism of action may lead to embarrassment, causing patients to avoid seeking treatment and contributing to late presentation. As of 2001, 1331 cases were reported in the literature. The incidence of concomitant urethral injury is 20%. [8]
An emerging trend is penile fracture following the use of collagenase clostridium histolyticum (CCH) injections for the treatment of Peyronie disease. The rate of penile fracture associated with CCH is reported to range from 0.5% to 4.9%, with a small fraction occurring spontaneously, in the absence of sexual activity. [9, 10]
Penile amputation
Penile amputation is rare, with most cases being reported sporadically. Cases are typically associated with self-mutilation related to acute psychotic episodes or gender dysphoria. Felonious assaults account for the remainder of cases.
Penetrating injury
Gunshot wounds account for 35% of all genital injuries. In 25% of cases, the penis alone is involved. In another 25% of cases, both the penis and scrotum are involved. Penetrating penile injury with concomitant urethral injury has been reported in 11–29% of cases. The frequency of stab wounds to the penis is relatively rare, accounting for only 4% of penetrating penile injuries.
Historically, wounds to the GU structures have been less common than extremity and penetrating abdominal trauma in combat operations. The use of improvised explosive devices (IEDs) has resulted in a significant increase in genitourinary (GU) wounds since 2001. Studies report that 20-31% of GU injuries involved the penis. [11, 12]
Penile soft tissue injury
Soft tissue skin loss of the penis is a rare phenomenon. Fournier gangrene accounts for approximately 75% of cases that involve genital skin loss. This infectious process is beyond the scope of this article and discussed in Fournier Gangrene. The remainder of soft tissue loss cases are typically due to avulsion injuries, human or animal bites, and burns.
Pubic hair grooming–related injuries, including lacerations and burns, have been reported, with the penis the second most common site of injury (34.8%). A cross-sectional study of US adults found 66.5% of men reporting a history of pubic hair grooming, with 23.7% having sustained an injury. Although most injuries reported were minor, 1.4% required medical attention. Men who removed all their pubic hair had an increased risk for grooming injury. [13]
Prognosis
Penile fracture
Penile fracture is a urologic emergency that may have devastating physiologic and psychologic consequences. However, with prompt diagnosis and expedient surgical management, outcomes remain excellent and complications are minimal. [14] Patients treated with conservative management have a significantly higher incidence of complications compared with those treated with prompt surgical therapy.
Potential complications of penile fracture include erectile dysfunction (which may result from a cavernosospongiosal fistula), abnormal penile curvature, painful erections, formation of fibrotic plaques, penile abscess, urethrocutaneous fistula, corporourethral fistula, and painful nodules along the site of injury.
Penile amputation
Erectile function remains in up to 86% of patients who undergo microvascular reanastomosis of the dorsal arteries. Penile sensation is maintained in up to 82% of patients, although this may be diminished when compared with preinjury. Urethral strictures develop in up to 20% of patients. Skin loss occurs in approximately half of all patients but is often superficial. Penile skin necrosis was more common prior to microvascular anastomosis of the dorsal neurovascular complexes. The necrosis that typically occurs is less frequent and often superficial.
Similar to the possible complications following correction of penile fracture, penile amputation can be associated with penile curvature, erectile dysfunction, hematoma, abscess formation, urethrocutaneous fistula, and corporourethral fistula.
Penetrating injury
Patients who undergo exploration and primary repair of penetrating penile injury have good outcomes. Potency is maintained in up to 80-100% of patients in some series. This depends on the degree and severity of injury. Some authors anecdotally report that patients who have suffered close-range shotgun blasts have poorer outcomes secondary to massive tissue destruction.
Similar to the possible complications following correction of penile fracture, penetrating corpora cavernosal injuries carry with them complications of erectile dysfunction, penile curvature, fibrotic plaques, abscess, and painful erections. Patients with urethral injuries risk corporourethral fistula, urethral stricture, and urethrocutaneous fistula.
Penile soft tissue injury
The long-term results of soft tissue injury to the penis are somewhat limited. Outcomes depend on the mechanism of injury and volume of tissue loss. Wound contracture and cosmesis is a concern in those who undergo skin grafting. If the graft does not take in patients who undergo split-thickness skin grafting, the consequences can be devastating. Penile sensation is decreased in those with significant penile skin loss.
The most frequent complication of soft tissue injury is postoperative infection; complications such as erectile dysfunction, curvature, and fistula are associated risks.
-
Eggplant deformity.
-
Small penile fracture involving the right corpus cavernosum.
-
More severe penile fracture.
-
Gunshot wound to the penis.
-
Partial penile amputation.
-
Repair of partial penile amputation after primary closure (without replantation of penile remnant).
-
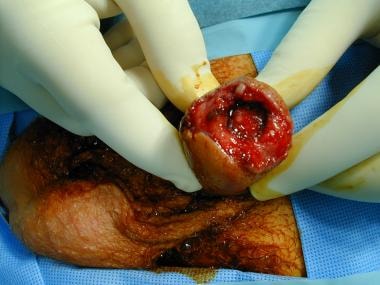
Penile amputation in the initial stage of replantation.
-
Penile amputation after replantation.
-
Presentation of superficial vascular injuries can be similar to penile fracture. Courtesy of Joel Gelman, MD.
-
Ligation of the injured superficial dorsal vein upon exploration. Courtesy of Joel Gelman, MD.
-
Concomitant urethral injury with visible Foley catheter.







