Background
The most likely causes of pediatric congestive heart failure depend on the age of the child. Congestive heart failure in the fetus, or hydrops, can be detected by performing fetal echocardiography. In this case, congestive heart failure may represent underlying anemia (eg, Rh sensitization, fetal-maternal transfusion), arrhythmias (usually supraventricular tachycardia), or myocardial dysfunction (myocarditis or cardiomyopathy). Curiously, structural heart disease is rarely a cause of congestive heart failure in the fetus, although it does occur. Atrioventricular valve regurgitation in the fetus is a particularly troubling sign with respect to the prognosis. (See Etiology.)
Neonates and infants younger than age 2 months are the most likely group to present with congestive heart failure related to structural heart disease. The systemic or pulmonary circulation may depend on the patency of the ductus arteriosus, especially in patients presenting in the first few days of life. In these patients, prompt cardiac evaluation is mandatory. Myocardial disease due to primary myopathic abnormalities or inborn errors of metabolism must be investigated. Respiratory illnesses, anemia, and known or suspected infection must be considered and appropriately managed. (See Etiology, Presentation, Workup, and Treatment.)
In older children, congestive heart failure may be caused by left-sided obstructive disease (valvar or subvalvar aortic stenosis or coarctation), myocardial dysfunction (myocarditis or cardiomyopathy), hypertension, renal failure, [1] or, more rarely, arrhythmias or myocardial ischemia. Illicit drugs such as inhaled cocaine and other stimulants are increasingly precipitating causes of congestive heart failure in adolescents; therefore, an increased suspicion of drug use is warranted in unexplained congestive heart failure. (See Etiology and Presentation.)
Although congestive heart failure in adolescents can be related to structural heart disease (including complications after surgical palliation or repair), it is usually associated with chronic arrhythmia or acquired heart disease, such as cardiomyopathy.
Patient education
For patient education information, see the Heart Health Center, as well as Congestive Heart Failure.
Etiology
Congestive heart failure occurs when the heart can no longer meet the metabolic demands of the body at normal physiologic venous pressures. Typically, the heart can respond to increased demands by means of 1 of the following:
-
Increasing the heart rate, which is controlled by neural and humoral input
-
Increasing the contractility of the ventricles, secondary to circulating catecholamines and autonomic input
-
Augmenting the preload, medicated by constriction of the venous capacitance vessels and the renal preservation of intravascular volume
As the demands on the heart outstrip the normal range of physiologic compensatory mechanisms, signs of congestive heart failure occur. These signs include tachycardia; venous congestion; high catecholamine levels; and, ultimately, insufficient cardiac output with poor perfusion and end-organ compromise. (See the image below.)
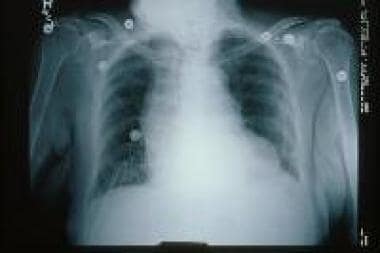 Chest radiograph shows signs of congestive heart failure (CHF).
Chest radiograph shows signs of congestive heart failure (CHF).
Systolic dysfunction
Diminished cardiac output is caused by a complex interaction of various factors. [2] Systolic dysfunction is characterized by diminished ventricular contractility that results in an impaired ability to increase the stroke volume to meet systemic demands. Factors such as anatomic stresses (eg, coarctation of the aorta) that contribute to an increased afterload (end-systolic wall stress), as well as neurohormonal factors that increase systemic vascular resistance, also lead to systolic dysfunction.
Diastolic dysfunction
Diastolic dysfunction results from decreased ventricular compliance, necessitating an increase in venous pressure to maintain adequate ventricular filling. Causes of primary diastolic dysfunction include an anatomic obstruction that prevents ventricular filling (eg, pulmonary venous obstruction), a primary reduction in ventricular compliance (eg, cardiomyopathy, transplant rejection), external constraints (eg, pericardial effusion), and poor hemodynamics after the Fontan procedure (eg, elevated pulmonary vascular resistance).
Chronic heart failure
In chronic heart failure, myocardial cells die from energy starvation, from cytotoxic mechanisms leading to necrosis, or from the acceleration of apoptosis or programmed cell death. Necrosis stimulates fibroblast proliferation, which results in the replacement of myocardial cells with collagen. The loss of myocytes leads to cardiac dilation and an increased afterload and wall tension, which results in further systolic dysfunction. In addition, the loss of mitochondrial mass leads to increased energy starvation.
Acute heart failure
During acute congestive heart failure, the sympathetic nervous system and renin-angiotensin system act to maintain blood flow and pressure to the vital organs. Increased neurohormonal activity results in increased myocardial contractility, selective peripheral vasoconstriction, salt and fluid retention, and blood pressure maintenance. As a chronic state of failure ensues, these same mechanisms cause adverse effects.
The myocardial oxygen demand, which exceeds the supply, increases because of an increase in the heart rate, in contractility, and in wall stress. Alterations in calcium homeostasis and changes in contractile proteins occur, resulting in a hypertrophic response of the myocytes. Neurohormonal factors may lead to direct cardiotoxicity and necrosis.
Characteristic findings in children with heart failure
Many classes of disorders can result in increased cardiac demand or impaired cardiac function. Cardiac causes include arrhythmias (tachycardia or bradycardia), structural heart disease, and myocardial dysfunction (systolic or diastolic).
Noncardiac causes of congestive heart failure include processes that increase the preload (volume overload), increase the afterload (hypertension), reduce the oxygen-carrying capacity of the blood (anemia), or increase demand (sepsis). For example, renal failure can result in congestive heart failure due to fluid retention and anemia. Renal failure may also occur following heart transplantation as a result of long-term immunosuppression. [3]
Cardiac rhythm disorders may be caused by the following:
-
Complete heart block
-
Supraventricular tachycardia
-
Ventricular tachycardia
-
Sinus node dysfunction
Volume overload may be caused by the following:
-
Structural heart disease (eg, ventricular septal defect, [4] patent ductus arteriosus, aortic or mitral valve regurgitation, complex cardiac lesions)
-
Anemia
-
Sepsis
Pressure overload may be caused by the following:
-
Structural heart disease (eg, aortic or pulmonary stenosis, aortic coarctation)
-
Hypertension
Systolic ventricular dysfunction or failure may be caused by the following:
-
Myocarditis
-
Dilated cardiomyopathy
-
Malnutrition
-
Ischemia
Diastolic ventricular dysfunction or failure may be caused by the following:
-
Hypertrophic cardiomyopathy
-
Restrictive cardiomyopathy
-
Pericarditis
-
Cardiac tamponade (pericardial effusion)
-
Chest radiograph shows signs of congestive heart failure (CHF).
Tables
Agent |
Pediatric Dose |
Comment |
Preload Reduction |
||
Furosemide |
1 mg/kg/dose PO or IV |
May increase to qid |
Hydrochlorothiazide |
2 mg/kg/d PO divided bid |
May increase to qid |
Metolazone |
0.2 mg/kg/dose PO |
Used with loop diuretic, may increase to bid |
Inotropic |
||
Digoxin |
Preterm infants: 0.005 mg/kg/d PO divided bid or 75% of this dose IV; age 10 y: 0.005 mg/kg/d PO qd or 75% of this dose IV |
... |
Dopamine |
5-10 mcg/kg/min IV (usual dosage; maximal dosage may be up to 28 mcg/kg/min) |
Gradually titrate upward to desired effect |
Dobutamine |
5-10 mcg/kg/min IV |
Gradually titrate upward to desired effect |
Epinephrine |
0.01-0.03 mcg/kg/min IV |
Not to exceed 0.1-0.3 mcg/kg/min |
Milrinone |
0.3-1 mcg/kg/min IV |
Typically used without loading dose, especially in unstable patients Load: 50 mcg/kg IV over 15 min |
Afterload Reduction |
||
Captopril |
0.1-0.5 mg/kg/d PO divided q8h |
... |
Enalapril |
0.1 mg/kg/d PO divided qd/bid, not to exceed 0.5 mg/kg/d |
Adults: 2.5-5 mg/day PO qd/bid initially; titrate slowly at 1- to 2-wk intervals; target dose is 10-20 mg PO bid; not to exceed 40 mg/day |
Lisinopril |
Not established |
Adults: Usual dosage is 10mg PO qd (range, 2.5-10 mg) |
Losartan |
Initial dose for hypertension is 0.1 mg/kg/day PO; dosage for treatment of CHF is not established in children |
Adults: 25-100 mg/d PO qd or divided bid |
Nitroprusside |
0.5-10 mcg/kg/min IV |
May need to monitor cyanide level |
Nitroglycerin |
0.1-0.5 mcg/kg/min IV |
Vasodilator |
Nesiritide |
0.01-0.03 mcg/kg/min IV |
Initiate with 0.01 mcg/kg/min May cause dose-related hypotension |
Alprostadil* |
0.03-0.1 mcg/kg/min IV |
... |
Beta-Blockade [7] |
||
Carvedilol |
Limited data suggest a therapeutic dosage range of 0.2-0.4 mg/kg/dose PO bid; initiate with lower dose and gradually increase dose q2-3wk to therapeutic range |
Adults: 12.5-25 mg PO bid Initiate with 3.125 mg PO bid |
Metoprolol |
Not established |
Adults: 25-100 mg PO qd |
Selective Aldosterone Antagonists |
||
Spironolactone |
1-3.3 mg/kg/day PO in single or divided doses |
Adults: 12.5-50 mg PO qd; reduce dose to 25 mg qod if hyperkalemia occurs |
Eplerenone |
Not established |
25-50 mg PO qd |
I(f) Current Inhibitor |
||
Ivabradine |
Initial >6 mo and < 40 kg: 0.05 mg/kg PO BID Maximum: 0.2 mg/kg BID (6 mo-1 y); 0.3 mg/kg BID (1 y or older) |
Lowers heart rate |
*Prostaglandin E1 (PGE1). |
||
Drug Class |
Recommendation |
Reduced EF (systolic HF) |
Preserved EF (diastolic HF) |
Diuretics |
Class I |
Patients with fluid retention associated with ventricular dysfunction (HF Stage C) to achieve a euvolemic state |
All patients to establish a euvolemic state |
Class I |
Perform close monitoring of renal function and blood pressure during initiation and up-titration of diuretic therapy |
||
Class IIa |
Consider diuretics to treatment systemic hypertension to prevent disease progression. |
||
Ace Inhibitors |
Class I (LoE B) |
For symptomatic left ventricular dysfunction (HF Stage C), use ACE inhibitors routinely unless there is a specific contraindication. Start at low doses and up-titrate to a maximum tolerated safe dose |
|
Class IIa (LoE B) |
For asymptomatic left ventricular dysfunction (HF Stage B), use ACE inhibitors routinely unless there is a specific contraindication. |
||
Class III (LoE B) |
Do not routinely use for patients with single-ventricle CHD, but could be considered in specific cases such as in situations of valve regurgitation or ventricular dysfunction |
||
Angiotensin antagonists |
Class IIa |
Generally reserved for systemic ventricular systolic dysfunction in patients who are intolerant of ACE inhibitors |
|
Class IIb |
Routine use is not recommended unless there is an additional indication such as hypertension. |
||
Class IIb |
May be used for control of hypertension but careful monitoring of hemodynamics and renal function is required due to the enhanced risk of hypotension and renal toxicity. |
||
Beta- Blockers |
Class IIa (LoE B) |
Consider beta-blockers in symptomatic children with systemic LV systolic dysfunction, particularly if the systemic ventricle has a LV morphology. Therapy should start at a small dose and slowly up-titrate |
|
Class IIa (LoE B) |
Consider beta-blockers in asymptomatic children with systemic LV systolic dysfunction. Therapy should start at a small dose and slowly up-titrate |
||
Calcium Channel Blockers |
Class III |
Not recommended unless there is an additional indication. |
|
Inotropic Agents |
Class III |
Use of intermittent or chronic inotropic therapy, other than as a bridge to transplant, is not recommended. |
|
Nesiritide |
Class IIb |
Not recommended for routine use although it may be considered in select patients where other interventions to lower central venous pressure have been unsuccessful. |

What would you like to print?
- Overview
- Presentation
- Workup
- Treatment
- Guidelines
- Medication
- Medication Summary
- Diuretics, Loop
- Diuretics, Thiazide
- Diuretics, Other
- Aldosterone Antagonists, Selective
- Inotropic Agents
- Alpha/Beta Adrenergic Agonists
- Prostaglandins, Endocrine
- ACE Inhibitors
- Angiotensin II Receptor Blockers (ARBs)
- Vasodilators
- Beta-Adrenergic Blockers
- I(f) Current Inhibitors
- Cardiovascular, Others
- Show All
- Tables
- References



