Background
Second-degree atrioventricular (AV) block occurs when regular atrial electrical impulse (ie, non-premature atrial systoles) fails to conduct to the ventricles. Second-degree AV block may occur in many different patterns, and the block may be physiologically located at any level between the atria and ventricles. Second-degree AV block is not a disease in and of itself; it is a pattern of cardiac rhythm that is most typically recognized on electrocardiogram (ECG).
On the basis of certain ECG characteristics, second-degree AV block is divided into Mobitz I AV block (or Wenckebach AV block) and Mobitz II AV block (or non-Wenckebach (fixed) AV block). This classification has clinical and prognostic implications. (See Prognosis and Presentation.)
Multiple disease entities are associated with second-degree AV block, which is frequently an intermediate finding between normal AV conduction and third-degree (ie, complete) AV block. (See Etiology.)
Although AV conduction delay may occur at multiple levels within the heart, it is typically observed in the specialized conduction system in the AV node (supra-Hisian), the His bundle (intra-Hisian), or the His bundle branches (infra-Hisian). Because these tissues have significant differences in their predominant ion channel currents, structure, and other features, the location of the block tends to be relatively disease-specific. In addition, the intrinsic pacemaker rate below the level of the block is sequentially slower in each tissue, making distal block of more concern than proximal block.
In second-degree AV block, the QRS duration is normal unless baseline bundle branch block is also present.
Mobitz I (Wenckebach) AV block
The most common pattern of Wenckebach second-degree AV block consists of progressive prolongation of the PR interval in consecutive beats leading up to a nonconducted P wave; this pattern is known as Mobitz I (Wenckebach) AV block. Mobitz I (Wenckebach) AV block may occur normally in the presence of increased vagal tone, such as in athletes or during sleep. However, a small number of patients may have AV node disease or a progressive conduction system disorder. Mobitz I AV block is also pathologic when it occurs during exercise. In classic Mobitz I (Wenckebach) block, the PR interval prolongs by sequentially smaller increments. Therefore, the RR intervals shorten prior to the blocked beat. However, only a minority of cases of Mobitz I (Wenckebach) block are classic.
Mobitz I (Wenckebach) block (see the image below) is often most easily diagnosed by comparing the PR interval after the blocked beat with the PR interval preceding the blocked beat. If the PR interval shortens following the blocked beat, the block is most likely of the Wenckebach type. However, if every other P wave is blocked, then the following interval is the same as the preceding interval, and the block cannot be designated as the Wenckebach type. In such cases, the block is simply designated as 2:1 AV block.
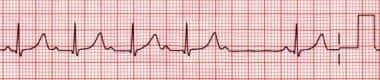 A common pattern of second-degree atrioventricular (AV) block consists of gradual prolongation of the PR interval leading up to a nonconducted P wave; this pattern is known as Wenckebach AV block, or Mobitz I AV block. This rhythm strip is an example of classic Mobitz I, or Wenckebach, AV block, in which the PR interval prolongs by sequentially smaller increments, with consequent shortening of the RR intervals until the blocked beat occurs. However, classic Wenckebach block is present in only a minority of cases. Wenckebach block is most easily diagnosed by comparing the PR interval following the blocked beat with the PR interval preceding the blocked beat; if the PR interval shortens following the blocked beat, the block is most likely of the Wenckebach type.
A common pattern of second-degree atrioventricular (AV) block consists of gradual prolongation of the PR interval leading up to a nonconducted P wave; this pattern is known as Wenckebach AV block, or Mobitz I AV block. This rhythm strip is an example of classic Mobitz I, or Wenckebach, AV block, in which the PR interval prolongs by sequentially smaller increments, with consequent shortening of the RR intervals until the blocked beat occurs. However, classic Wenckebach block is present in only a minority of cases. Wenckebach block is most easily diagnosed by comparing the PR interval following the blocked beat with the PR interval preceding the blocked beat; if the PR interval shortens following the blocked beat, the block is most likely of the Wenckebach type.
When Mobitz I (Wenckebach) block is assessed by means of invasive electrophysiologic (EP) study, the block is most commonly found to be high in the specialized AV conduction system, usually above the bundle of His in the compact AV node area. The classic intracardiac EP finding is progressive AH interval lengthening until the atrial depolarization fails to conduct to the ventricles. The escape rates are usually somewhat faster and more reliable than in infra-Hisian block.
Mobitz II (non-Wenckebach) AV block
Mobitz II (non-Wenckebach) AV block (see the image below) may be diagnosed when there is no progressive prolongation of the PR interval and the PR interval fails to shorten following a blocked beat. This block is usually located more distally in the His bundle or bundle branches, or both than that seen in Mobitz I, and the escape rates are usually slower and less stable than in Mobitz I block. The intracardiac EP recording will show similar AH intervals, with sudden failure to conduct to the ventricles.
 If there is no progressive prolongation of the PR interval and the PR interval fails to shorten following a blocked beat, non-Wenckebach AV block (or Mobitz II AV block) is said to be present. This block is usually located more distally in the His bundle or the His bundle branches, or both, and the escape rates are usually slower and less stable.
If there is no progressive prolongation of the PR interval and the PR interval fails to shorten following a blocked beat, non-Wenckebach AV block (or Mobitz II AV block) is said to be present. This block is usually located more distally in the His bundle or the His bundle branches, or both, and the escape rates are usually slower and less stable.
High-grade AV block
High-grade AV block is present when more than two consecutive P waves do not conduct. These P waves fall beyond the T wave and not during the refractory period and thus should conduct under normal circumstances. However, occasionally, P waves do conduct. Therefore, the ventricular rate is neither regular nor completely dissociated. The implications of high-grade AV block appear to be similar to those of complete AV block.
Patient education
Discuss the possibility of permanent pacing systems early with patients who are likely to require them. This allows patients and their families sufficient time to accommodate the concept of living with a pacemaker. Identify misconceptions and dispel myths (which are often present) related to living with a pacemaker.
Etiology
The causes of second-degree AV block are often the same diseases that cause congenital or acquired complete AV block. These diseases include autoimmune or inflammatory conditions, such as neonatal lupus erythematosus, myocarditis, endocarditis, Lyme disease, and rheumatic fever.
Toxicity from drugs or other substances also frequently causes second-degree AV block. Such toxicities include excessive doses of digoxin, beta blockers, calcium channel blockers, and Vaughan Williams class III agents (eg, sotalol, amiodarone).
Thyroid diseases are a frequent cause of second-degree AV block, particularly the Mobitz I (Wenckebach) type, possibly because of hyperthyroidism (eg, thyrotoxicosis, which is sometimes exacerbated by beta-blocker therapy) or hypothyroidism, either primary or drug-induced.
A subgroup of infants with congenital long QT syndrome may present with 2:1 AV block, presumably related to the His-Purkinje system or to ventricular myocardial refractoriness. In these patients, the ventricular tissue fails to repolarize sufficiently early for all P waves to be conducted. The 2:1 AV block can often be initiated or terminated by atrial or ventricular extrastimuli that are appropriately timed, spontaneous, or induced. The unique pattern may be recognized even in utero. The QT interval may be long and may be associated with a high risk of infant mortality. Therapy with beta blockers and pacing has been recommended, but such therapy has shown only partial success.
Mechanical
Surgery-related blocks range from first-degree to third-degree. Prolonged cross-clamp time may increase the incidence of postoperative AV block. [1] When advanced, second-degree and third-degree AV blocks persist for more than 7 days after surgery, permanent pacing is indicated.
Postcatheterization first-degree, second-degree, or third-degree AV block can occur, especially in patients with corrected transposition of the great arteries in which the AV node has an anterior and superior location and a long, penetrating common bundle that travels toward the ventricle along the anterior edge of the pulmonary valve. Therefore, it can be easily traumatized by catheter movement when trying to cross the pulmonary valve.
With placement of an atrial septal defect (ASD) occluder device, second-degree AV block may occur, especially when a large device is required in cases with a large ASD. [2]
With radiofrequency (RF) ablation, AV block may be transient and may subside when edema and inflammation in the AV node–His region subside, or it may be permanent because of inadvertent ablation of the conduction tissue in that region.
Tumor-related AV block may occur in cases of rhabdomyoma involving the AV conduction system. Patients with Duchenne muscular dystrophy may develop second-degree AV block. Conduction system abscesses secondary to endocarditis may lead to any degree of AV block.
Second-degree AV block may be seen in acute rheumatic heart disease and Lyme carditis (due to Borrelia burgdorferi). Mobitz I (Wenckebach) AV block during recovery from dengue hemorrhagic fever has been reported and may be a transient functional impairment of the AV node in which an altered autonomic tone may play a role. [3]
Scorpion bites can provoke serious arrhythmic events and hemodynamic disturbance, with disturbance of sympathetic and parasympathetic balance.
Immunologic
Newborns may present with second-degree and third-degree AV block secondary to passive transfer of maternal anti-SSA/Ro and anti-SSB/La antibodies. This can occur either in mothers with autoimmune disease or in asymptomatic mothers who have positive titers for those antibodies. [4]
Because progression to more advanced degrees of AV block can occur, electrocardiography should be performed on all infants born to mothers with anti-SSA/Ro and anti-SSB/La antibodies.
One study reported that when isolated second-degree AV block is detected in a fetus without structural cardiac anomalies and the mother is seronegative for anti-SSA/Ro and anti-SSB/La antibodies, a high likelihood of reverting to sinus rhythm by the time of delivery was observed. [5] This is in contrast to what occurs when second-degree AV block is detected in a fetus with structural cardiac anomalies, tachyarrhythmia, nonconducted premature atrial beats, or long QT syndrome or when mothers are seropositive for anti-SSA/Ro and anti-SSB/La antibodies.
Genetic
Patients with long QT syndrome may have second-degree AV block due to exceedingly long repolarization time, rendering the ventricle refractory to the next atrial depolarization wave.
Progressive familial heart block of Mobitz type II is a rare autosomal dominant trait in which first-degree AV block progresses to second-degree and third-degree AV block and, sometimes, to dilated cardiomyopathy with age. Affected individuals characteristically have sinus bradycardia at a ventricular rate of less than 50 beats per minute.
Diseases due to mutations in the lamin A/C gene (LMNA) include neuromuscular and cardiac dystrophies, lipodystrophies, and premature aging syndromes. [6] Patients with the heterozygous LMNA R482W mutation, which is the most frequent genotype associated with familial partial lipodystrophy of the Dunnigan type (FPLD), have muscular and cardiac abnormalities with a limb-girdle muscular dystrophy, cardiac hypertrophy, rhythm disturbances (such as second-degree AV block), and advanced atherosclerosis.
Another rare cause of second-degree AV block is familial amyloidosis with polyneuropathy, in which extracellular amyloid infiltration of the heart produces sinus node dysfunction, conduction disturbances, cardiomyopathy, and congestive heart failure. [7]
Kearns-Sayre syndrome is a mitochondrial cytopathy that manifests itself in persons younger than 20 years with pigmentary retinopathy, chronic progressive external ophthalmoplegia, and one or more of the following: cardiac conduction defects, cerebellar ataxia, and cerebrospinal fluid protein concentration greater than 1 g/L (100 mg/dL). A single large mitochondrial deoxyribonucleic acid (DNA) deletion of 4977 bp is the most common molecular defect.
Inheritance of Kearns-Sayre syndrome is matrilinear; therefore, all offspring (males and females) of affected women, but none of affected men, are at risk. Because sudden death in these patients is attributed to sudden onset of complete cardiac block, a prophylactic pacemaker should be implanted whenever second-degree AV block or bifascicular block develops.
Sickle cell disease and sickle cell trait have a high prevalence in the black population. Transient Wenckebach and non-Wenckebach AV block due to localized ischemia in the AV node and the His bundle area has been described during a severe sickle cell crisis. Therefore, if second-degree AV block is encountered during a sickle cell crisis, potentially lethal complications (eg, massive myocardial infarction) should be prevented, if possible, with prompt and aggressive treatment of the crisis.
Drug-induced QT prolongation
Antiarrhythmic medications in this category include disopyramide, dofetilide, ibutilide, procainamide, quinidine, sotalol, bepridil, and amiodarone.
Other drugs that may prolong the QT interval include anti-infective agents such as clarithromycin, erythromycin, halofantrine, pentamidine, and sparfloxacin; antiemetic agents such as domperidone and droperidol; antipsychotic agents such as chlorpromazine, haloperidol, mesoridazine, thioridazine, and pimozide; cisapride; lidoflazine; and methadone.
Susceptibility to develop drug-induced torsade de pointes is higher in females; in the presence of hypokalemia, bradycardia, or recent conversion from atrial fibrillation (especially with a QT-prolonging drug); in congestive heart failure; with concomitant digitalis therapy; with elevated drug concentrations (with the exception of quinidine); in cases of rapid rate of intravenous infusion with the QT-prolonging drug; and in the presence of baseline QT prolongation, subclinical long-QT syndrome, ion-channel polymorphisms, or severe hypomagnesemia.
More information on various drugs linked to torsades de pointes may be found at CredibleMeds.org.
Post–heart transplant
One study reported that although first-degree, second-degree, and third-degree AV block may develop after orthotopic heart transplant, first-degree AV block is more likely to be related to cellular rejection and coronary artery disease–induced atrial conduction disturbance, whereas second-degree and third-degree AV blocks are mainly the consequences of surgical and catheter intervention injury. [8]
Epidemiology
The frequency of second-degree AV block in the general population is unknown, but isolated Mobitz I (Wenckebach) AV block occurring during sleep is recognized to be a frequent and normal physiologic finding. Second-degree AV block occurring at other times or in other patterns may be abnormal, and the potential causes are multiple and rare.
Sex-related demographics
No sex predilection for second-degree AV block was known until an international study that included a large number of first-grade and junior-high-school subjects found that rhythm disturbances, including first-degree, second-degree, and third-degree AV block, were more prevalent in males. [9]
Age-related demographics
Second-degree AV block can occur at any age; it is seen during fetal monitoring and through infancy, childhood, and adulthood. [10]
Second-degree AV block may be detected in a fetus with or without structural cardiac anomalies whose mother is seronegative or seropositive for anti-SSA/Ro and anti-SSB/La antibodies. In fetuses, second-degree and third-degree AV blocks are often associated with complex and changing atrial and ventricular rhythms. [11]
International studies done in children have found that rhythm disturbances, including first-degree, second-degree, and third-degree AV block, increase with age. [9, 12]
Progressive familial heart block of Mobitz type II is a rare entity in which first-degree AV block progresses to second-degree and third-degree AV block and, sometimes, to dilated cardiomyopathy. Progression occurs in late adolescence or young adulthood. [13] Therefore, establishing a family history and performing periodic (ie, yearly) ECG and clinical evaluations in patients with asymptomatic first-degree and second-degree AV block may be warranted.
Prognosis
With the severe infantile form of long-QT syndrome, the prognosis is very guarded, even if patients are treated with beta blockade, pacing, and stellate ganglionectomy. The prognosis of patients with high-grade AV block is similar to that of patients with complete AV block.
The implications of second-degree AV block depend on the underlying cause, its potential for progression to complete AV block, and the location and rate of the potential subsidiary pacemaker.
Fetal bradyarrhythmia associated with congenital heart defects has a poor prognosis. [14]
-
A common pattern of second-degree atrioventricular (AV) block consists of gradual prolongation of the PR interval leading up to a nonconducted P wave; this pattern is known as Wenckebach AV block, or Mobitz I AV block. This rhythm strip is an example of classic Mobitz I, or Wenckebach, AV block, in which the PR interval prolongs by sequentially smaller increments, with consequent shortening of the RR intervals until the blocked beat occurs. However, classic Wenckebach block is present in only a minority of cases. Wenckebach block is most easily diagnosed by comparing the PR interval following the blocked beat with the PR interval preceding the blocked beat; if the PR interval shortens following the blocked beat, the block is most likely of the Wenckebach type.
-
If there is no progressive prolongation of the PR interval and the PR interval fails to shorten following a blocked beat, non-Wenckebach AV block (or Mobitz II AV block) is said to be present. This block is usually located more distally in the His bundle or the His bundle branches, or both, and the escape rates are usually slower and less stable.





