Practice Essentials
Malnutrition is directly responsible for 300,000 deaths per year in children younger than 5 years in developing countries and contributes indirectly to more than half of all deaths in children worldwide. In addition, it increases health care costs. See the image below.
 This infant presented with symptoms indicative of Kwashiorkor, a dietary protein deficiency. Note the angular stomatitis indicative of an accompanying Vitamin B deficiency as well. Image courtesy of the Centers for Disease Control and Prevention.
This infant presented with symptoms indicative of Kwashiorkor, a dietary protein deficiency. Note the angular stomatitis indicative of an accompanying Vitamin B deficiency as well. Image courtesy of the Centers for Disease Control and Prevention.
See 23 Hidden Clues to Diagnosing Nutritional Deficiencies, a Critical Images slideshow, to help identify clues to conditions associated with malnutrition.
Signs and symptoms
History
According to the American Society for Parenteral and Enteral Nutrition (ASPEN), malnutrition can be classified as either being illness related (secondary to another disease or injury) non-illness related, (attributable to environmental/behavioral causes) or a combination of the two. [1]
The most common and clinically significant micronutrient deficiencies and their consequences include the following:
-
Iron: Fatigue, anemia, decreased cognitive function, headache, glossitis, and nail changes
-
Iodine: Goiter, developmental delay, and intellectual disability
-
Vitamin D: Poor growth, rickets, and hypocalcemia
-
Vitamin A: Night blindness, xerophthalmia, poor growth, and hair changes
-
Folate - Glossitis, anemia (megaloblastic), and neural tube defects (in fetuses of women without folate supplementation)
-
Zinc: Anemia, dwarfism, hepatosplenomegaly, hyperpigmentation and hypogonadism, acrodermatitis enteropathica, diminished immune response, and poor wound healing
Physical examination
Physical findings that are associated with protein-energy malnutrition (PEM) include the following [2] :
-
Decreased subcutaneous tissue: Areas that are most affected are the legs, arms, buttocks, and face
-
Edema: Areas that are most affected are the distal extremities and anasarca (generalized edema)
-
Oral changes: Cheilosis, angular stomatitis, and papillar atrophy
-
Abdominal findings: Abdominal distention secondary to poor abdominal musculature and hepatomegaly secondary to fatty infiltration
-
Skin changes: Dry, peeling skin with raw, exposed areas; hyperpigmented plaques over areas of trauma
-
Nail changes: Fissured or ridged nails
-
Hair changes: Thin, sparse, brittle hair that is easily pulled out and that turns a dull brown or reddish color
See Clinical Presentation for more detail.
Diagnosis
Initial diagnostic laboratory studies include the following:
-
Complete blood cell count
-
Sedimentation rate
-
Serum electrolytes
-
Urinalysis
-
Culture
Stool specimens should be obtained if the child has a history of abnormal stools or stooling patterns or if the family uses an unreliable or questionable source of water.
The most helpful laboratory tests for assessing malnutrition in a child are hematologic and protein status studies.
Hematologic studies
Hematologic studies should include a complete blood count with red blood cell indices and a peripheral smear.
Protein studies
Measures of protein nutritional status include levels of the following:
-
Serum albumin
-
Retinol-binding protein:
-
Prealbumin:
-
Transferrin
-
Creatinine
-
Blood urea nitrogen
Additional laboratory studies
Other studies may focus on thyroid functions or sweat chloride tests, particularly if height velocity is abnormal.
Nutritional status studies
Practical nutritional assessment includes the following:
-
Complete history, including a detailed dietary history
-
Growth measurements, including weight and length/height; head circumference in children younger than 3 years
-
Complete physical examination
See Workup for more detail.
Management
Children with chronic malnutrition may require caloric intakes of more than 120-150 kcal/kg/day to achieve appropriate weight gain. Most children with mild malnutrition respond to increased oral caloric intake and supplementation with vitamin, iron, and folate supplements. The requirement for increased protein is met typically by increasing the food intake. Management must be carried out in centers by physicians familiar with nutritional disorders as nutritional recovery syndrome may include excessive sweating and hepatomegaly. Refeeding syndrome is a potentially life threatening condition that occurs with administration of high calorie feeds in severely malnourished children. This potentially fatal condition is associated with electrolyte disturbances including hypokalemia and hypophosphatemia
In moderate to severe cases of malnutrition, enteral supplementation via tube feedings may be necessary.
Prevention
The prevention of malnutrition in children starts with an emphasis on prenatal nutrition and good prenatal care. Promotion of breastfeeding is particularly crucial in developing countries where safe alternatives to human milk are unavailable. Health care providers should also counsel parents on the appropriate introduction of nutritious supplemental foods.
See Treatment for more detail.
Background
The World Health Organization defines malnutrition as "the cellular imbalance between supply of nutrients and energy and the body's demand for them to ensure growth, maintenance, and specific functions." [3] More recently, the American Society for Parenteral and Enteral Nutrition (ASPEN) workgroup defined pediatric malnutrition [undernutrition] as "an imbalance between nutrient requirement and intake, resulting in cumulative deficits of energy, protein, or micronutrients that may negatively affect growth, development, and other relevant outcomes." [1] Women and young children are the most adversely affected groups; one quarter to one half of women of child-bearing age in Africa and south Asia are underweight, which contributes to the number of low birth weight infants born annually. [4]
Malnutrition is globally the most important risk factor for illness and death, contributing to more than half of deaths in children worldwide; child malnutrition was associated with 54% of deaths in children in developing countries in 2001. [3, 4] Protein-energy malnutrition (PEM), first described in the 1920s, is observed most frequently in developing countries but has been described with increasing frequency in hospitalized and chronically ill children in the United States. [5] . However, consensus guidelines now address malnutrition irrespective of etiology. ASPEN identified two alternative ways to diagnose malnutrition: BMI and unintentional weight loss. Among the various guidelines, the Subjective Global Assessment [SGA] is a highly validated tool which includes medical history and a physical assessment. [6] The main classification of malnutrition is either illness based [severe or moderate] or Non-illness based [severe to moderate] and were recently addressed. [7]
The effects of changing environmental conditions in increasing malnutrition is multifactorial. Poor environmental conditions may increase insect and protozoal infections and also contribute to environmental deficiencies in micronutrients. Overpopulation, more commonly seen in developing countries, can reduce food production, leading to inadequate food intake or intake of foods of poor nutritional quality. Conversely, the effects of malnutrition on individuals can create and maintain poverty, which can further hamper economic and social development. [4]
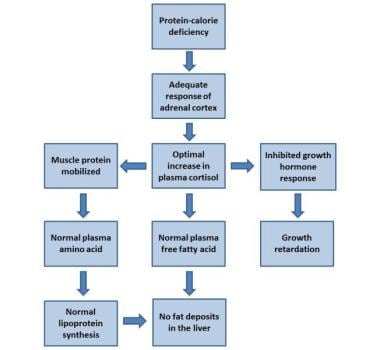
Kwashiorkor and marasmus are 2 forms of PEM that have been described but there has been a paradigm shift in diagnosing pediatric malnutrition. The new schema for defining malnutrition incorporates the concepts of chronicity, etiology, and pathogenesis of malnutrition; its relationship with inflammation; and its impact on functional outcomes. [1] The distinction between the 2 forms of PEM is based on the presence of edema (kwashiorkor) or absence of edema (marasmus). Marasmus involves inadequate intake of protein and calories, whereas a child with kwashiorkor has fair-to-normal calorie intake with inadequate protein intake. Although significant clinical differences between kwashiorkor and marasmus are noted, some studies suggest that marasmus represents an adaptation to starvation whereas kwashiorkor represents a dysadaptation to starvation. See the image below.
This infant presented with symptoms indicative of Kwashiorkor, a dietary protein deficiency. Note the angular stomatitis indicative of an accompanying Vitamin B deficiency as well. Image courtesy of the Centers for Disease Control and Prevention.
In addition to PEM, children may be affected by micronutrient deficiencies, which also have a detrimental effect on growth and development. The most common and clinically significant micronutrient deficiencies in children and childbearing women throughout the world include deficiencies of iron, iodine, zinc, and vitamin A and are estimated to affect as many as two billion people. Although fortification programs have helped diminish deficiencies of iodine and vitamin A in individuals in the United States, these deficiencies remain a significant cause of morbidity in developing countries, whereas deficiencies of vitamin C, B, and D have improved in recent years. Micronutrient deficiencies and protein and calorie deficiencies must be addressed for optimal growth and development to be attained in these individuals.
Pathophysiology
Malnutrition affects virtually every organ system. Dietary protein is needed to provide amino acids for synthesis of body proteins and other compounds that have various functional roles. Energy is essential for all biochemical and physiologic functions in the body. Furthermore, micronutrients are essential in many metabolic functions in the body as components and cofactors in enzymatic processes.
In addition to the impairment of physical growth and of cognitive and other physiologic functions, immune response changes occur early in the course of significant malnutrition in a child. These immune response changes correlate with poor outcomes and mimic the changes observed in children with acquired immune deficiency syndrome (AIDS). Loss of delayed hypersensitivity, fewer T lymphocytes, impaired lymphocyte response, impaired phagocytosis secondary to decreased complement and certain cytokines, and decreased secretory immunoglobulin A (IgA) are some changes that may occur. These immune changes predispose children to severe and chronic infections, most commonly, infectious diarrhea, which further compromises nutrition causing anorexia, decreased nutrient absorption, increased metabolic needs, and direct nutrient losses.
Early studies of malnourished children showed changes in the developing brain, including, a slowed rate of growth of the brain, lower brain weight, thinner cerebral cortex, decreased number of neurons, insufficient myelinization, and changes in the dendritic spines. More recently, neuroimaging studies have found severe alterations in the dendritic spine apparatus of cortical neurons in infants with severe protein-calorie malnutrition. These changes are similar to those described in patients with intellectual disability of different causes. There have not been definite studies to show that these changes are causal rather than coincidental. [8]
Other pathologic changes include fatty degeneration of the liver and heart, atrophy of the small bowel, and decreased intravascular volume leading to secondary hyperaldosteronism.
Etiology
Inadequate food intake is the most common cause of malnutrition worldwide. In developing countries, inadequate food intake is secondary to insufficient or inappropriate food supplies or early cessation of breastfeeding. In some areas, cultural and religious food customs may play a role. Inadequate sanitation further endangers children by increasing the risk of infectious diseases that increase nutritional losses and alters metabolic demands.
In developed countries, inadequate food intake is a less common cause of malnutrition. Instead, diseases and, in particular, chronic illnesses play an important role in the etiology of malnutrition. Children with chronic illness are at risk for nutritional problems for several reasons, including the following:
-
Children with chronic illnesses frequently have anorexia, which leads to inadequate food intake.
-
Increased inflammatory burden and increased metabolic demands can increase caloric need.
-
Any chronic illness that involves the liver or small bowel affects nutrition adversely by impairing digestive and absorptive functions.
Chronic illnesses that commonly are associated with nutritional deficiencies include the following:
-
Chronic renal failure
-
Childhood malignancies
-
Congenital heart disease
-
Neuromuscular diseases
-
Chronic inflammatory bowel diseases
In addition, the following conditions place children at significant risk for the development of nutritional deficiencies:
-
Prematurity
-
Developmental delay
-
In utero toxin exposure (ie, fetal alcohol exposure)
Children with multiple food allergies present a special nutritional challenge because of severe dietary restrictions. Patients with active allergic symptoms may have increased calorie and protein needs.
Guidelines on fruit juice intake for children by the American Academy of Pediatrics recommend that in the evaluation of children with malnutrition, the pediatrician should determine the amount of juice being consumed as excessive juice consumption may be associated with malnutrition (overnutrition and undernutrition). [9]
Epidemiology
United States statistics
Fewer than 1% of all children in the United States have chronic malnutrition. Incidence of malnutrition is less than 10%, even in the highest risk group (children in shelters for the homeless). Some studies indicate that poor growth secondary to inadequate nutrition occurs in as many as 10% of children in rural areas. Studies of hospitalized children suggest that as many as one fourth of patients had some form of acute PEM and 27% had chronic PEM.
International statistics
The World Health Organization estimates that by the year 2015, the prevalence of malnutrition will have decreased to 17.6% globally, with 113.4 million children younger than 5 years affected as measured by low weight for age. The overwhelming majority of these children, 112.8 million, will live in developing countries with 70% of these children in Asia, particularly the southcentral region, and 26% in Africa. An additional 165 million (29.0%) children will have stunted length/height secondary to poor nutrition.
Currently, more than half of young children in South Asia have PEM, which is 6.5 times the prevalence in the western hemisphere. In sub-Saharan Africa, 30% of children have PEM. Despite marked improvements globally in the prevalence of malnutrition, rates of undernutrition and stunting have continued to rise in Africa, where rates of undernutrition and stunting have risen from 24% to 26.8% and 47.3% to 48%, respectively, since 1990, with the worst increases occurring in the eastern region of Africa. [3]
Children are most vulnerable to the effects of malnutrition in infancy and early childhood. Premature infants have special nutritional needs that are not met with traditional feeding recommendations; they require fortified human milk or specially designed preterm formula until later in infancy. Children are susceptible to malnutrition for differing reasons. During adolescence, self-imposed dietary restrictions contribute to the incidence of nutritional deficiencies.
Paradoxically, a massive global epidemic of obesity, especially in countries in rapid economic transition, is simultaneously emerging in children and adolescents. The concurrent manifestation of both undernutrition and overweight/obesity has been termed the double burden of malnutrition (DBM). The greatest concentration of the DBM is found in sub-Saharan Africa, South Asia, and East Asia and the Pacific region. [10]
Prognosis
Children who have chronic malnutrition, especially those with intrauterine growth retardation and with onset at an early age, do not achieve their full growth potential or regain cognitive deficits. Although malnutrition is rare in the United States and other industrialized countries, over half of childhood mortality in developing countries is either directly or indirectly secondary to malnutrition.
Morbidity/mortality
Malnutrition is directly responsible for 300,000 deaths per year in children younger than 5 years in developing countries and contributes indirectly to more than half the deaths in childhood worldwide.
The adverse effects of malnutrition include physical and developmental manifestations. Poor weight gain and slowing of linear growth occur. Impairment of immunologic functions in these children mimics those observed in children with AIDS, predisposing them to opportunistic and other typical childhood infections.
In developing countries, poor perinatal conditions account for 23% of deaths in children younger than five. Malnourished women are at high risk of giving birth to low birth weight infants. Many low birth weight infants (15-20% of all births worldwide) [11] face severe short-term and long-term health consequences, such as growth failure in infancy and childhood, which increases risk of morbidity and early death. [4]
Children who are chronically malnourished exhibit behavioral changes, including irritability, apathy and decreased social responsiveness, anxiety, and attention deficits. In addition, infants and young children who have malnutrition frequently demonstrate developmental delay in delayed achievement of motor skills, delayed mental development, and may have permanent cognitive deficits. The degree of delay and deficit depends on the severity and duration of nutritional compromise and the age at which malnutrition occurs. In general, nutritional insults at younger ages have worse outcomes. Dose-dependent relationships between impaired growth and poor school performance and decreased intellectual achievement have been shown. [4, 12, 13, 14]
Although death from malnutrition in the United States is rare, in developing countries, more than 50% of the 10 million deaths each year are either directly or indirectly secondary to malnutrition in children younger than 5 years. [3] A meta-analysis by Karunaratne et al identified six independent factors associated with mortality in children hospitalized for complicated severe acute malnutrition: HIV infection, diarrhea, pneumonia, shock, lack of appetite, and lower weight-for-height z score. [15]
-
Hormonal adaptation to the stress of malnutrition: The evolution of marasmus.
-
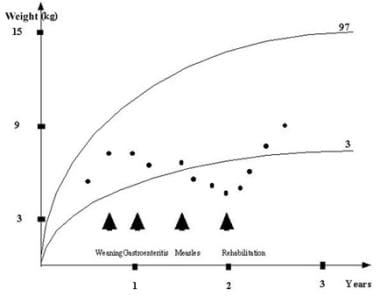
A classic example of a weight chart for a severely malnourished child.
-
This infant presented with symptoms indicative of a dietary protein deficiency, including edema and ridging of the toenails. Image courtesy of the Centers for Disease Control and Prevention.
-
This infant presented with symptoms indicative of Kwashiorkor, a dietary protein deficiency. Note the angular stomatitis indicative of an accompanying Vitamin B deficiency as well. Image courtesy of the Centers for Disease Control and Prevention.





