Background
Neurologic manifestations are among the features of systemic lupus erythematosus (SLE), a multisystem autoimmune connective tissue disorder with various clinical presentations. SLE affects many organ systems, including the central and peripheral nervous systems and muscles. [1]
Central nervous system (CNS) lupus is a serious but potentially treatable illness, which can present with significant diagnostic challenges (see the following image). This condition is in the differential diagnosis for many neurologic conditions. Thus, neurologists and other clinicians need to be aware of the various presentations and neurologic complications of SLE; patients with SLE often have neurologic symptoms, and rarely, SLE is diagnosed after patients present for treatment of a neurologic event. [2, 3]
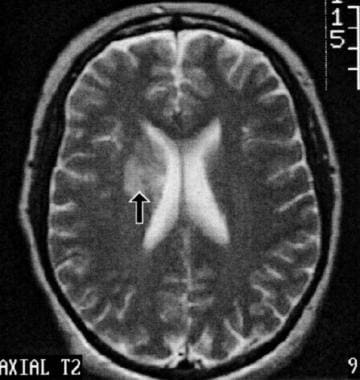 This axial, T2-weighted brain magnetic resonance image (MRI) demonstrates an area of ischemia in the right periventricular white matter of a 41-year-old woman with longstanding systemic lupus erythematosus (SLE). She presented with headache and subtle cognitive impairments but no motor deficits. Faintly increased signal intensity was also seen on T1-weighted images, with a trace of enhancement following gadolinium that is too subtle to show on reproduced images. The distribution of the abnormality is consistent with occlusion of deep penetrating branches, such as may result from local vasculopathy, with no clinical or laboratory evidence of lupus anticoagulant or anticardiolipin antibody. Cardiac embolus from covert Libman-Sacks endocarditis remains less likely due to the distribution.
This axial, T2-weighted brain magnetic resonance image (MRI) demonstrates an area of ischemia in the right periventricular white matter of a 41-year-old woman with longstanding systemic lupus erythematosus (SLE). She presented with headache and subtle cognitive impairments but no motor deficits. Faintly increased signal intensity was also seen on T1-weighted images, with a trace of enhancement following gadolinium that is too subtle to show on reproduced images. The distribution of the abnormality is consistent with occlusion of deep penetrating branches, such as may result from local vasculopathy, with no clinical or laboratory evidence of lupus anticoagulant or anticardiolipin antibody. Cardiac embolus from covert Libman-Sacks endocarditis remains less likely due to the distribution.
See also Pediatric Systemic Lupus Erythematosus, Neonatal and Pediatric Lupus Erythematosus, Systemic Lupus Erythematosus and Pregnancy, Discoid Lupus Erythematosus, Bullous Systemic Lupus Erythematosus (BSLE), Acute Cutaneous Lupus Erythematosus (ACLE), Subacute Cutaneous Lupus Erythematosus (SCLE), and Physical Medicine and Rehabilitation for Systemic Lupus Erythematosus.
Pathophysiology
The pathophysiology of SLE has not been fully defined, although many genes that affect immune function, particularly the variants in human leukocyte antigen (HLA), may augment susceptibility to clinical disease. Most monozygotic (identical) twins are discordant for clinical SLE, strongly suggesting that additional factors, probably environmental, trigger the widespread development of autoimmunity in susceptible individuals.
Certain medications (e.g., phenytoin, hydralazine, procainamide, and isoniazid) can produce drug-induced lupus. However, this disorder differs from the classic SLE in its autoantibody profile (e.g., anti-histone antibody positivity) and in sparing the kidneys and CNS. Once triggered, SLE's autoimmune reaction affects many organ systems. Various mechanisms such as deposition of immune complexes, effects of cytokines and other chemical neuromodulators, direct attack by autoantibodies or activated leukocytes, play a role in tissue injury and destruction.
Non-neurologic sites of damage include the renal glomeruli, joints, pleural or pericardial serosa, integument, cardiac or vascular endothelium, cardiac valves, and the oral and conjunctival mucosa. Multiple sites may be involved within the nervous system.
Etiology
Among the neurologic manifestations of systemic lupus erythematosus (SLE), the most common are the organic encephalopathies. Functional studies such as positron emission tomography (PET) scanning, functional magnetic resonance imaging (fMRI), or single-photon emission computerized tomography (SPECT) scanning demonstrate patchy areas of dysfunction in brain areas not demonstrable on conventional MRI. These findings suggest an uncoupling of metabolic processes independent of obstruction to cerebral blood flow. The mechanism of these metabolic alterations is unknown. (See CT Scanning and MRI.)
In areas of apparent vasculitis, histology demonstrates degenerative changes in small vessel walls, often with minimal or no inflammatory infiltrates. Chronic effects of immune complex deposition offer one potential mechanism for SLE vasculopathy; cytokine-mediated effects on vascular endothelium or local brain parenchyma are another. Inflammatory and noninflammatory SLE vasculopathy may be clinically indistinguishable. The terms cerebritis and vasculitis are well embedded in the literature and will be used in this article, keeping in mind the evolving understanding of the underlying processes.
In addition to small vessel vasculopathy, inflammatory changes may occur in large- to medium-sized vessels, giving a more classic vasculitis, sometimes with clinical stroke syndromes resulting from local thrombosis or artery-to-artery emboli. Other potential stroke etiologies include local thrombosis from antiphospholipid antibodies, which may involve small or medium-sized arteries or veins, including the venous sinuses.
Emboli can occur due to Libman-Sacks endocarditis (LSE), a sterile endocardial inflammation that produces vegetations on the heart valves, seen in greater frequency in the presence of antiphospholipid antibodies. LSE may also cause a diffuse microembolization pattern that is clinically hard to distinguish from vasculitis or cerebritis. In focal clinical syndromes, overt or covert cardiac emboli are more frequently responsible than focal vasculitis or thrombotic processes. (See Biopsies and Histologic Features.)
Antiphospholipid antibodies comprise one category of the multiple autoantibodies that are associated with SLE. In addition to their association with LSE and local arterial or venous thrombosis, these antibodies also may be associated with hemorrhagic diathesis, myelopathy, and non-neurologic manifestations such as spontaneous abortion.
Dural sinus thrombosis is a rare complication of SLE-associated hypercoagulability and is often seen in association with antiphospholipid antibodies. Radiologically, flow defects in one or more venous sinuses may be imaged with MRI, MR venous angiography, conventional angiography, or radionuclide brain scanning. Associated edema or hemorrhagic infarcts may be evident on MRI or CT scans.
Drug-induced myopathy
The most common type of drug-induced myopathy is steroid-induced myopathy. It usually presents with progressing painless muscle weakness, fatigability, and muscle atrophy, and is an adverse effect of glucocorticoid use (though fluorinated glucocorticoid has a higher chance of causing this).
Muscle biopsy often reveals slight variation in fiber size with type 2b atrophy, with little or no fiber necrosis and no inflammatory cells. Biopsy also often reveals a slight myofibrillar loss with accumulations of glycogen, lipids, and aggregates of mitochondria. (See Biopsies and Histologic Features).
Amphiphilic drug myopathies
Amphiphilic drug myopathies are often caused by drugs with hydrophobic moiety and the hydrophilic region containing an amine group. They produce multisystem disorders including neuropathy, myopathy, and cardiomyopathy. Chloroquine and hydroxychloroquine cause vacuolar myopathy, often given in a 500 mg daily dose of chloroquine for one year or longer. At extracellular pH, this drug is poorly ionized and penetrates membranes. With acid pH in lysosomes, the cationic region interacts with polar materials.
Muscle biopsy reveals vacuoles with lipid and membranous material, with strong acid phosphatase staining in muscle fibers and normal periodic acid-Schiff (PAS) staining for glycogen. (See Biopsies and Histologic Features.)
Epidemiology
According to a set of definitions of 19 neuropsychiatric systemic lupus erythematosus (NPSLE) syndromes and their diagnostic criteria from the American College of Rheumatology (ACR), less than 40-50% of events are due to underlying CNS lupus activity (primary NPSLE). The rest are indirectly associated with the disease and can be the consequence of metabolic disturbances, infections, or drug effects (secondary NPSLE). [4, 5, 6]
Data from large cohorts suggest prevalence rates of approximately 30–40% for NPSLE. [7, 8] Further studies show NPSLE is at least as common in children as it is in adults. [9, 10]
A three-year prospective study of 370 SLE patients with no previous history of CNS involvement determined that clinically severe CNS involvement is rare in SLE patients, accounting only for 7.8 per 100 person-years. [11]
Prognosis
The neuropsychiatric events in systemic lupus erythematosus (SLE) appear to have a more favorable outcome than events secondary to non-SLE causes. Events attributed to SLE generally occur during the early course of the illness, do have a negative impact on the quality of life of the patient, and vary in both severity and frequency. [5]
Neurologic complications worsen prognosis, especially in the presence of refractory seizures, encephalopathy, or paralysis from stroke or myelopathy.
Taddio et al concluded that the presence of atypical manifestations of pediatric SLE at presentation and early kidney disease correlated with poor outcomes. Similarly, during follow-up, kidney and CNS diseases were associated with worse outcome. [12]
-
This axial, T2-weighted brain magnetic resonance image (MRI) demonstrates an area of ischemia in the right periventricular white matter of a 41-year-old woman with longstanding systemic lupus erythematosus (SLE). She presented with headache and subtle cognitive impairments but no motor deficits. Faintly increased signal intensity was also seen on T1-weighted images, with a trace of enhancement following gadolinium that is too subtle to show on reproduced images. The distribution of the abnormality is consistent with occlusion of deep penetrating branches, such as may result from local vasculopathy, with no clinical or laboratory evidence of lupus anticoagulant or anticardiolipin antibody. Cardiac embolus from covert Libman-Sacks endocarditis remains less likely due to the distribution.
Tables

What would you like to print?
- Overview
- Presentation
- DDx
- Workup
- Approach Considerations
- Serum Chemistry Studies
- Hepatocellular and Muscle Enzyme Levels
- Antinuclear Antibody Test
- Lupus Anticoagulant Test
- CSF Studies
- Brain Imaging Studies
- Spinal Imaging Studies
- Echocardiography and Ultrasonography
- Electroencephalography
- EMG and Nerve Conduction Studies
- Biopsies and Histologic Features
- Show All
- Treatment
- Medication
- Questions & Answers
- References





