Practice Essentials
Approximately 40-50 species of venomous coral snakes exist in North America and South America, with the greatest variety from Mexico to northern South America. A number of African and Asian coral snake species also exist. All coral snakes belong to the family Elapidae; Micrurus fulvius (eastern coral snake) and Micrurus tener (Texas coral snake) are the most important species in the United States.
Another US coral snake, Micruroides euryxanthus (Sonoran or Arizona coral snake), is a small and relatively innocuous snake, and no deaths have been attributed to its bite.
Coral snakes tend to be relatively shy creatures, and bites are uncommon. Coral snakes account for less than 1% of venomous snakebites in the United States. Most people bitten by coral snakes are handling them intentionally. Most bites occur in the spring or fall. Deaths have been reported but are extremely rare.
History
Also see Physical Examination.
The vast majority of patients bitten by coral snakes report that a brightly colored snake bit them.
North of Mexico City, including the United States, the color pattern of the snake can be helpful in differentiating a coral snake from a harmless mimic (eg, nonvenomous milk snake). In this region, all coral snakes have a red, yellow, black, yellow, red banding pattern (every other band is yellow; red and yellow bands touching, and bands completely encircle the body; see the image below); most harmless mimics have a red, black, yellow, black, red pattern (every other band is black; red and yellow separated by black; and/or some bands do not completely encircle the body). [1] The mnemonic "Red on yellow, kill a fellow; red on black, venom lack," may be helpful in this region. South of Mexico City, this rule can not be used as the banding patterns are much different, and bicolor (red and black) species are also present.
 Snake envenomations, coral. Comparison of the harmless Lampropeltis triangulum annulata(Mexican milksnake) (top) with Micrurus tener(Texas coral snake) (bottom). Photo by Charles Alfaro.
Snake envenomations, coral. Comparison of the harmless Lampropeltis triangulum annulata(Mexican milksnake) (top) with Micrurus tener(Texas coral snake) (bottom). Photo by Charles Alfaro.
History may include the following:
-
Onset of symptoms may be delayed up to 10-12 hours but may then be rapidly progressive.
-
Paucity of local complaints
-
Local paresthesias (may be painful)
-
Soft tissue swelling (usually mild)
-
Myalgias have been reported
-
Alteration of mental status
-
Complaints related to cranial nerve dysfunction (eg, diplopia, ptosis, difficulty swallowing)
Complications
Complications of snake bite may include the following:
-
Respiratory failure
-
Aspiration
-
Cardiovascular collapse
-
Prolonged neuromuscular weakness
Diagnostics
No laboratory studies are of diagnostic benefit. Baseline laboratory studies (eg, complete blood count [CBC], electrolyte tests, renal function studies) may be obtained in severe bite cases or if the patient has significant underlying medical problems. Coagulation studies are not indicated.
An arterial blood gas (ABG) determination may be helpful if the patient's respiratory status is of concern.
A chest radiograph is beneficial in patients who have severe envenomation, who require intubation, or who show evidence of cardiopulmonary failure.
If available, pulmonary function testing such as negative inspiratory force (NIF) and forced vital capacity (FVC) can be used to determine if patients may have impending respiratory failure. Similarly, the single breath count (SBC) test can also be used. To perform the SBC: Ask the patient to take a deep breath and count as high as possible in their normal speaking voice without taking another breath. A normal SBC is approximately 50 and SBC < 20 is associated with the need for mechanical ventilation. [2]
Treatment
See Prehospital Care, Emergency Department Care, and Medication.
Consult a toxicologist, poison control center, or an expert in snakebite management.
Complications
Antivenom-related complications may include anphylatic reactions, anphylactoid reactions and delayed serum sickness. These can range from mild (rash) to life-threatening (hypotension, shock).
Long-term monitoring
Muscle weakness can takes weeks to resolve. Follow up with primary care physicain or a medical toxicologist is recommended after discharge.
Prevention
Avoid handling venomous or unidentified snakes.
Use caution when placing bare hands or feet into areas where one cannot see and in which snakes may be seeking shelter.
Pathophysiology
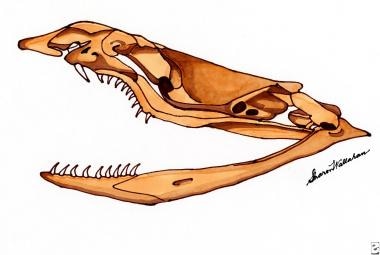
The coral snake venom apparatus is composed of a pair of small, fixed, hollow fangs in the anterior aspect of the upper jaw through which the snake injects venom via a chewing motion (see the image below). Unlike pit vipers, such as rattlesnakes, copperheads, and cottonmouths, which strike quickly, coral snakes must hang on for a brief period to achieve significant envenomation in humans.
Coral snake venoms tend to have significant neurotoxicity, inducing neuromuscular dysfunction. Coral snake venom has components which inhibit pre-synaptic releast of acetylcholinesterase and post-synaptic binding of acetylcholinesterase. They have little enzymatic activity or necrotic potential compared with most vipers and pit vipers. These venoms tend to be some of the most potent found in snakes, yet the venom yield per animal is less than that of most vipers or pit vipers. Because of the relatively primitive venom delivery apparatus, as many as 60% of those bitten by North American coral snakes are not envenomed (ie, they receive a "dry bite").
Epidemiology
United States
There were 76 alleged coral snake bites reported to the American Association of Poison Control Centers in 2020. [3]
International
No accurate information on international incidence is available, but there are no regions of the world where coral snake bites would be considered common. [4, 5]
Prognosis
With sound supportive care (eg, prevention of aspiration) and appropriate antivenom administration, when available, prognosis following coral snake envenomation is excellent and a full recovery is expected. This is generally true, even in the absence of an available, appropriate antivenom, [6] but the overall clinical course (including the need for prolonged intubation and respiratory support) will be longer. Patients who survive the bite may require respiratory support for up to a week and may suffer persistent weakness for weeks to months.
A single death has been reported due to a coral snake bite in the United States in the last 40 years (roughly, since coral snake antivenom became available). [7] Before that time, the estimated case-fatality rate was 10%, and the cause of death was respiratory or cardiovascular failure.
-
Snake envenomations, coral. Comparison of the harmless Lampropeltis triangulum annulata(Mexican milksnake) (top) with Micrurus tener(Texas coral snake) (bottom). Photo by Charles Alfaro.
-
Coral snake skull.
-
The Australian pressure immobilization technique: Step 1. This technique has been shown to be helpful in delaying systemic absorption of elapid venoms. A broad pressure bandage is immediately wrapped, beginning distally, around as much of the extremity as possible. No effort should be spent removing clothing prior to bandage application. The bandage is wrapped snugly, as for a severely sprained ligament. A splint (or sling when applied to the upper extremity) is then placed, and the victim is carried from the scene. The victim should expend no effort in getting to definitive care. Pressure immobilization should remain in place until the victim has reached medical care. The doctor will decide when to remove the bandages. If venom has been injected, it will move into the bloodstream quickly once the bandages are removed. The doctor should leave the bandages and splint in position until appropriate antivenom is available whenever possible. Used with permission from Commonwealth Serum Laboratories.
-
The Australian pressure immobilization technique: Step 2. This technique has been shown to be helpful in delaying systemic absorption of elapid venoms. A broad pressure bandage is immediately wrapped, beginning distally, around as much of the extremity as possible. No effort should be spent removing clothing prior to bandage application. The bandage is wrapped snugly, as for a severely sprained ligament. A splint (or sling when applied to the upper extremity) is then placed, and the victim is carried from the scene. The victim should expend no effort in getting to definitive care. Pressure immobilization should remain in place until the victim has reached medical care. The doctor will decide when to remove the bandages. If venom has been injected, it will move into the bloodstream quickly once the bandages are removed. The doctor should leave the bandages and splint in position until appropriate antivenom is available whenever possible. Used with permission from Commonwealth Serum Laboratories.
-
The Australian pressure immobilization technique: Step 3. This technique has been shown to be helpful in delaying systemic absorption of elapid venoms. A broad pressure bandage is immediately wrapped, beginning distally, around as much of the extremity as possible. No effort should be spent removing clothing prior to bandage application. The bandage is wrapped snugly, as for a severely sprained ligament. A splint (or sling when applied to the upper extremity) is then placed, and the victim is carried from the scene. The victim should expend no effort in getting to definitive care. Pressure immobilization should remain in place until the victim has reached medical care. The doctor will decide when to remove the bandages. If venom has been injected, it will move into the bloodstream quickly once the bandages are removed. The doctor should leave the bandages and splint in position until appropriate antivenom is available whenever possible. Used with permission from Commonwealth Serum Laboratories.
-
The Australian pressure immobilization technique: Step 4. This technique has been shown to be helpful in delaying systemic absorption of elapid venoms. A broad pressure bandage is immediately wrapped, beginning distally, around as much of the extremity as possible. No effort should be spent removing clothing prior to bandage application. The bandage is wrapped snugly, as for a severely sprained ligament. A splint (or sling when applied to the upper extremity) is then placed, and the victim is carried from the scene. The victim should expend no effort in getting to definitive care. Pressure immobilization should remain in place until the victim has reached medical care. The doctor will decide when to remove the bandages. If venom has been injected, it will move into the bloodstream quickly once the bandages are removed. The doctor should leave the bandages and splint in position until appropriate antivenom is available whenever possible. Used with permission from Commonwealth Serum Laboratories.
-
The Australian pressure immobilization technique: Step 5. This technique has been shown to be helpful in delaying systemic absorption of elapid venoms. A broad pressure bandage is immediately wrapped, beginning distally, around as much of the extremity as possible. No effort should be spent removing clothing prior to bandage application. The bandage is wrapped snugly, as for a severely sprained ligament. A splint (or sling when applied to the upper extremity) is then placed, and the victim is carried from the scene. The victim should expend no effort in getting to definitive care. Pressure immobilization should remain in place until the victim has reached medical care. The doctor will decide when to remove the bandages. If venom has been injected, it will move into the bloodstream quickly once the bandages are removed. The doctor should leave the bandages and splint in position until appropriate antivenom is available whenever possible. Used with permission from Commonwealth Serum Laboratories.








